EMBRYOLOGY
The pituitary gland is derived from two sources. The epithelial part, which includes the pars distalis, pars intermedia, and pars tuberalis, originates from an evagination of the stomodeal ectoderm called the Rathke pouch. The neural portion, which includes the pars infundibularis or infundibulum, the neural stalk, and the pars posterior or pars nervosa, arises from the floor of the diencephalon.
The Rathke pouch is detectable at approximately the third week of gestation as a small, thin-walled vesicle in the roof of the stomodeum, which is the primitive buccal cavity. After increasing in size, it adheres to the infundibulum. Its distal end becomes narrower and forms the craniopharyngeal canal, which subsequently is obliterated, although in some cases it may remain patent until the end of intrauterine life or even after birth. The anterior wall of its proximal portion, where cell replication is faster, gives rise to the pars distalis; the posterior wall develops to become the pars intermedia. The anterolateral part of the Rathke pouch grows upward on both sides, in front of the infundibulum, forming the pars tuberalis (Fig. 11-1).
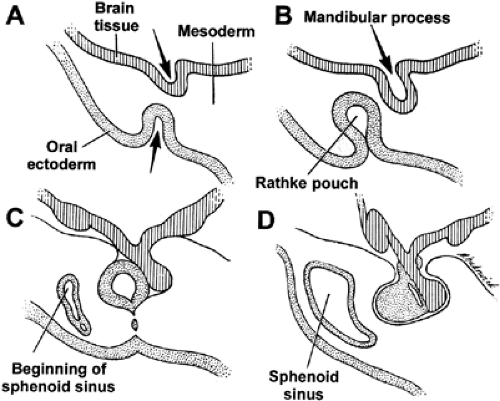 FIGURE 11-1. Embryogenesis of pituitary gland. A, Early invagination of primitive stomodeum and infundibular process. B, Growth of mesoderm constricts Rathke pouch. C, Further development pinches off Rathke pouch from oral cavity. D, Rathke cleft components develop into the pars distalis, pars tuberalis, and possibly the pars intermedia. Infundibular process develops into infundibular stalk and pars nervosa. (From Tindall GT, Barrow DL. Disorders of the Pituitary. St Louis: Mosby, 1986:10, with permission.) |
By the end of the third month of intrauterine life, the gross features of the pituitary gland are clearly recognizable. The infundibulum becomes elongated, and the pituitary is embedded deeper in the sella turcica. The neurohypophysis differentiates into the proximal median eminence and the distal posterior lobe, which are connected by the hypophysial stalk.
Pituitary hormones are synthesized early in embryonic life. In humans, growth hormone (GH) and adrenocorticotropic hormone (ACTH) can be demonstrated by immunocytology and radioimmunoassay at approximately the ninth week of gestation. These two hormones are soon followed by the appearance of the α and then the β subunits of glycoprotein hormones: thyroid-stimulating hormone (TSH), follicle-stimulating hormone (FSH), and luteinizing hormone (LH). Prolactin is the last adenohypophysial hormone to be produced; it can be detected at approximately the 20th week of intrauterine life. Vasopressin and oxytocin are found at ˜10 weeks of gestation.
Histologic differentiation also takes place early. Acidophilic cells are noticeable at approximately the third month of gestation; basophilic cells appear a little later. In approximately the eighth week of embryonic life, a large connective tissue mass carrying blood vessels to the developing anterior lobe becomes visible. The neurosecretory material in the posterior lobe can be recognized at approximately the fifth month of gestation.
ANATOMY
The pituitary lies in the sella turcica, or hypophysial fossa, at the base of the brain; it is surrounded by the sphenoid bone. The pituitary gland is an oval, bean-shaped, bilaterally symmetric organ measuring ˜13 mm transversely, 9 mm anteroposteriorly, and 6 mm vertically.
The average weight of the pituitary is 0.6 g; it ranges from 0.4 g to 0.8 g in adults, and averages 0.1 g at birth. A reduction in weight is evident in old age, and an increase occurs during pregnancy and lactation. The pituitary gland weighs somewhat
more in multiparous women than in nulliparous women or in men. The anterior lobe is larger than the posterior lobe, constituting ˜80% of the organ. The cut surface of the adenohypophysis is brownish red and can be distinguished from the sharply demarcated grayish neurohypophysis.
more in multiparous women than in nulliparous women or in men. The anterior lobe is larger than the posterior lobe, constituting ˜80% of the organ. The cut surface of the adenohypophysis is brownish red and can be distinguished from the sharply demarcated grayish neurohypophysis.
The pituitary is covered by the dura, a dense layer of connective tissue that lines the sella. The sella diaphragm, the connective tissue dura covering the superior surface of the sella, has a small central opening that is penetrated by the hypophysial stalk. The diameter of the opening is ˜5 mm.
Well protected in the bony sella, the pituitary is located in the vicinity of several structures. The lateral walls of the sella on both sides are close to the cavernous sinuses, the internal carotid arteries, and the oculomotor, trochlear, and abducent nerves. Below and in front of the sella lies the sphenoid sinus, which is separated from the sella by a thin layer of bone. Above the sellar diaphragm and in front of the hypophysial stalk is the optic chiasm. Above the roof of the sella is the median eminence, the hypothalamus, and the third ventricle of the brain.
Anatomically, the pituitary is divided into two different structures: the adenohypophysis, which consists of the pars distalis, the pars intermedia, and the pars tuberalis; and the neurohypophysis, which consists of the median eminence, the hypophysial stalk, and the pars posterior or pars nervosa. The pars distalis, the largest part of the adenohypophysis, is the main site of adenohypophysial hormone synthesis and discharge. In humans, the pars intermedia is rudimentary, and its functional significance is unknown. The pars tuberalis, the upward extension of the adenohypophysis, surrounds two sides of the hypophysial stalk and consists of adenohypophysial cells, primarily gonadotropes and thyrotropes. The pars nervosa, the downward extension of the brain, is connected to the hypothalamus by the hypophysial stalk (Fig. 11-2).
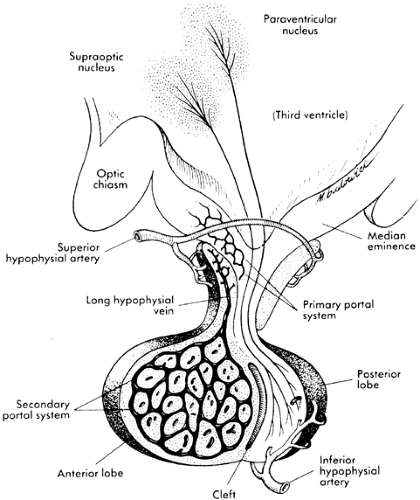 FIGURE 11-2. Sagittal diagram of the pituitary and its important anatomic features, including blood supply. (From Tindall GT, Barrow DL. Disorders of the Pituitary. St Louis: Mosby, 1986:11, with permission.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|