Androgen hypersecretion in postmenopausal women may be due to an ovarian tumor, an adrenal tumor, ovarian hyperthecosis, or nonclassic congenital adrenal hyperplasia. The expansiveness of the diagnostic evaluation of a woman with androgen excess is dependent on the clinical situation and the degree of androgen hypersecretion. When there is an abrupt onset of marked signs and symptoms and marked increases in serum testosterone concentrations, it is important to assess the patient with a full androgen profile and imaging studies of the ovaries and adrenal glands. When an adrenal tumor with a suspicious imaging phenotype is identified in a woman with androgen excess, it should be determined if other adrenocortical hormones are also being autonomously secreted. Herein we present an unusual case a pure testosterone-secreting adrenal adenoma.
Case Report
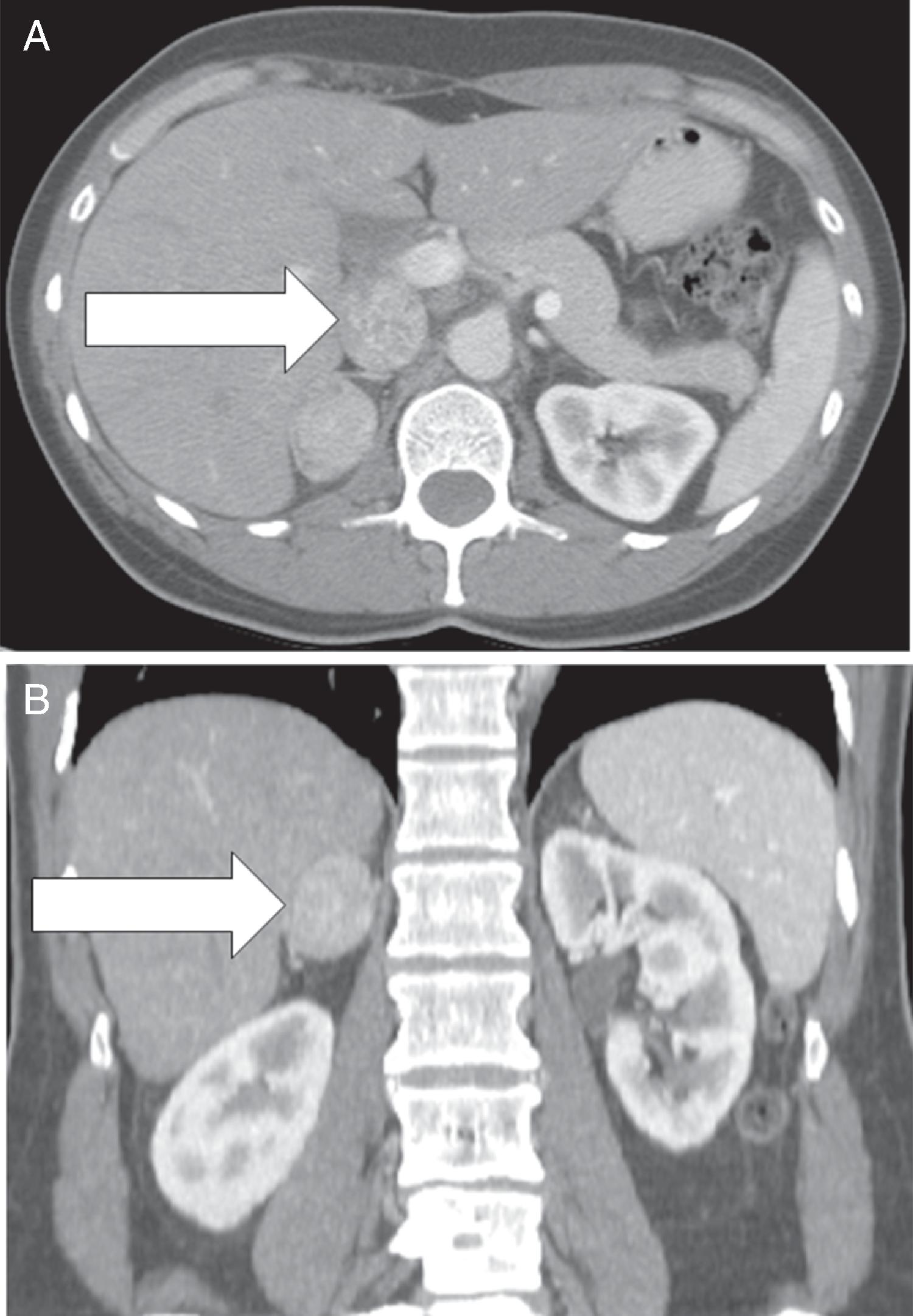
The patient was a 52-year-old woman who started noticing increasing facial hair 18 months before referral to Mayo Clinic. She was treated with laser therapy but found she had to repeat the treatment every 3 weeks. Over the past 1 year her symptoms progressed and she noticed new acne, temporal scalp hair recession, and increased hair on her breasts, abdomen, and back. She noticed that when she lifted weights that it took less weightlifting to maintain her muscle bulk and tone. She had also noted increased libido and enlargement of her clitoris. Three months before referral, serum testosterone was measured and found to be markedly elevated at 334 ng/dL (normal, 8–60 ng/dL), and this led to a computed tomography (CT) scan of the abdomen, which detected a 2.8 × 3.5–cm right adrenal mass ( Fig. 93.1 ). Her medical history was significant for total hysterectomy and bilateral salpingo-oophorectomy 5 years previously for the treatment of uterine fibroids (estrogen replacement therapy was initiated postoperatively). She was at ideal body weight. She had no signs or symptoms of Cushing syndrome. There was no history of hypokalemia. Her medications included piperazine estrone sulfate, 1.5 mg daily, and levothyroxine, 88 mcg daily.
On physical examination, her body mass index was 21.7 kg/m 2 , blood pressure 135/85 mmHg, and heart rate 57 beats per minute. She had marked hirsutism on her chin, abdomen, and pelvis. Her Ferriman-Gallwey score was 17 (normal, <8; maximum = 36). She also had mild androgenic scalp hair loss. External genitalia examination showed a prominent clitoris. There were no signs of glucocorticoid excess.
INVESTIGATIONS
Laboratory test results are shown in Table 93.1 . Marked testosterone and androstenedione hypersecretion was documented. The patient had testosterone-associated polycythemia. Measurements of glucocorticoids and mineralocorticoids were normal. Despite the suspicious imaging phenotype on CT scan, the monohormonal hypersecretion favored a benign testosterone-secreting adrenal adenoma.
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Lynch Syndrome
Adrenocortical Carcinoma Associated With Lynch Syndrome
 Metastatic Paraganglioma: Role for Systemic Chemotherapy
Metastatic Paraganglioma: Role for Systemic Chemotherapy
 Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
 Bilateral Macronodular Adrenal Hyperplasia in the Setting of Multiple Endocrine Neoplasia Type 1
Bilateral Macronodular Adrenal Hyperplasia in the Setting of Multiple Endocrine Neoplasia Type 1
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


