Chapter 37 T-Cell Lymphomas
Treatment of Peripheral T-Cell Lymphoma
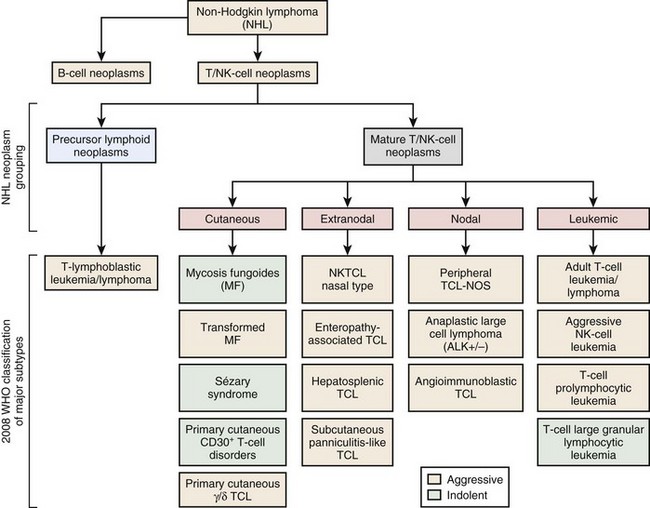
Figure 37-1 WHO CLASSIFICATION OF THE MATURE T-CELL NEOPLASMS.
NK, Natural killer; NOS, not otherwise specified; TCL, T-cell lymphoma.
Related posts:
 Heme Biosynthesis and Its Disorders: Sideroblastic Anemia
Heme Biosynthesis and Its Disorders: Sideroblastic Anemia
 Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 2
Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 2
 Thrombotic Thrombocytopenic Purpura and the Hemolytic Uremic Syndrome
Thrombotic Thrombocytopenic Purpura and the Hemolytic Uremic Syndrome
 Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 1
Infectious Mononucleosis and Other Epstein-Barr Virus–Associated Diseases: Part 1
 Disorders of Coagulation in the Neonate
Disorders of Coagulation in the Neonate
 Hypercoagulable States
Hypercoagulable States
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


