Postmenopausal androgen hypersecretion may be due to an ovarian tumor, an adrenal tumor, or ovarian hyperthecosis. It is important to assess the patient with a full androgen profile and imaging studies of the ovaries and adrenal glands. When an adrenal tumor is identified in a postmenopausal woman with androgen excess, adrenal and gonadal venous sampling may be needed to localize the source of androgen hypersecretion. Herein we present such a case.
Case Report
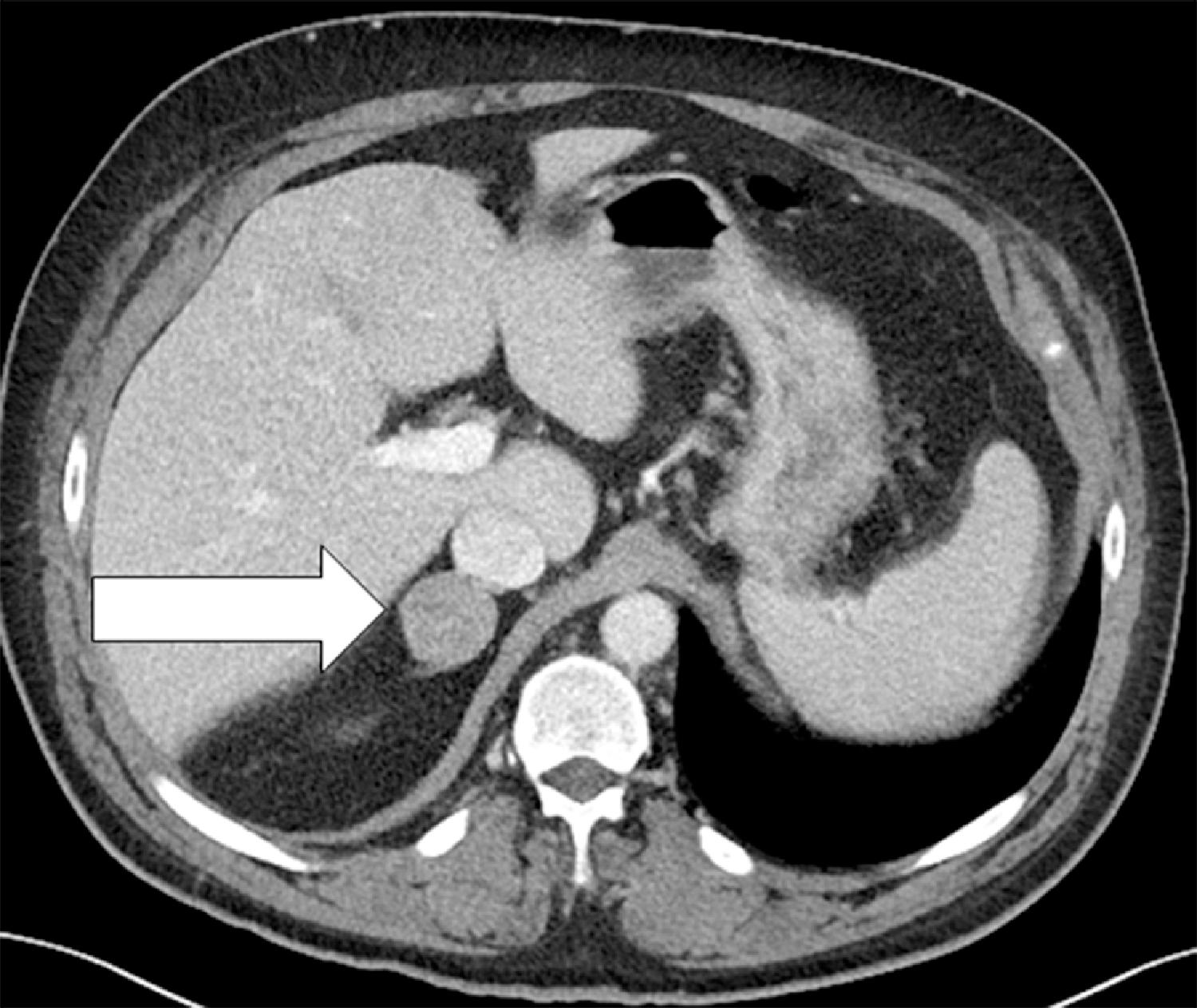
This 71-year-old woman had an abdominal computed tomography (CT) scan to investigate nonspecific abdominal discomfort, and a 3.4-cm right adrenal mass was incidentally discovered ( Fig. 92.1 ). She had no signs or symptoms of glucocorticoid or catecholamine hypersecretion. However, the patient had long-standing hirsutism primarily affecting the extremities and the suprapubic area. Starting 3 years previously, she experienced a steady and progressive increase in her hirsutism—affecting the whole anterior abdomen, anterior chest, chin, upper lip, and her back. She shaved her chin and upper lip every day and her abdomen and chest twice a week. She did not have acne or change in secondary sex characteristics or libido. She had two biologic children. Menopause occurred at 52 years of age, and she was not treated with estrogen or progesterone replacement. She had a 5-year history of hypertension treated with monotherapy (ramipril, 20 mg daily). There was no history of hypokalemia. On physical examination her body mass index was 31.8 kg/m 2 , blood pressure 142/70 mmHg, and heart rate 70 beats per minute. Her degree of hirsutism was marked with a modified Ferriman-Gallwey score of 33 (normal, <8; maximum = 36). Clitoromegaly was present (2.5 cm × 1 cm).
INVESTIGATIONS
Laboratory test results are shown in Table 92.1 . Pure testosterone hypersecretion was documented. Transabdominal and endovaginal ultrasound of the pelvis showed a 1.3-cm partially calcified fibroid in the uterine fundus and normal-appearing endometrial stripe, and both ovaries appeared normal. The question was whether the source of testosterone hypersecretion was adrenal or ovarian. Adrenal and gonadal venous sampling was the next step. Adrenal venous sampling was successful based on adrenal vein-to–inferior vena cava (IVC) cortisol gradients of more to 5-to-1 ( Box 92.1 ). The adrenal vein testosterone concentrations, proportionate to cortisol concentrations, were less than that in the IVC—confirming that the source of excess testosterone was not adrenal in origin. On the other hand, the testosterone concentrations in the right and left gonadal veins were 27-fold and 22-fold higher, respectively, than the testosterone concentration in the IVC (see Box 92.1 ). Bilateral ovarian testosterone hypersecretion was confirmed and consistent with hyperthecosis.
| Biochemical Test | Result | Reference Range |
| Sodium, mEq/L Potassium, mEq/L Creatinine, mg/dL Total testosterone, ng/dL Free testosterone, ng/dL Androstenedione, ng/dL DHEA-S, mcg/dL 17-Hydroxyprogesterone, ng/dL LH, IU/L FSH, IU/L Estradiol, pg/mL Aldosterone, ng/dL 1-mg overnight DST cortisol, mcg/dL 24-Hour urine cortisol, mcg | 142 4.9 1.2 417 60 89 39.5 91 22.1 71.1 11 7.9 1.8 6.1 | 135–145 3.6–5.2 0.6–1.1 8–60 0.3–1.9 30–200 15–157 Postmenopausal: <51 Postmenopausal: 5.3–65.4 Postmenopausal: 16–157 Postmenopausal: <10 ≤21 <1.8 mcg/dL 3.5–45 |
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Lynch Syndrome
Adrenocortical Carcinoma Associated With Lynch Syndrome
 Metastatic Paraganglioma: Role for Systemic Chemotherapy
Metastatic Paraganglioma: Role for Systemic Chemotherapy
 Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
 Bilateral Macronodular Adrenal Hyperplasia in the Setting of Multiple Endocrine Neoplasia Type 1
Bilateral Macronodular Adrenal Hyperplasia in the Setting of Multiple Endocrine Neoplasia Type 1
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


