SONOGRAPHY (ECHOGRAPHY) OF THE THYROID
In ultrasonography, high-frequency sound waves enter the body and are transmitted or reflected by tissue interfaces to produce a photographic image of the internal structure. With current high-resolution equipment, nodules as small as 2 to 3 mm can be identified by using a signal with a frequency of 7.5 to 10 MHz that penetrates <5 cm. The deeper penetration that is achieved by lower-frequency sound waves seldom is necessary for the evaluation of thyroid structures.3,4,4a
Patients are examined in the supine position with the neck hyperextended. For full imaging of the thyroid gland and appropriate landmarks, the neck must be surveyed in the sagittal, transverse, and oblique planes. The images are produced quickly and assembled in rapid sequence in “real time”, much as in a motion picture. Swallowing may facilitate identification of the esophagus; swallowing also elevates the thyroid so that its lower poles can be examined. A useful advance in thyroid ultrasonography is color flow Doppler imaging, which adds dynamic flow information to a static gray-scale image.4b Color-encoded signals differentiate a fluid-filled cystic space and vasculature, indicating the direction and the velocity of blood flow and the degree of vascularity.5 The assignment of color is arbitrary; arterial signals can be assigned the color red and the companion venous signals, blue, assuming that venous flow is parallel to, but in the opposite direction of, arterial flow. However, because vessels may be tortuous, portions of the same vessel may display in different colors depending on the direction of flow in relation to the transducer, even if the true direction of flow has not changed. The shade of a color is related roughly to flow velocity. The ultrasonography operator must be experienced and must be aware of the clinical question that has been posed by the clinician to provide an appropriate answer. Routine protocols for scanning are unsatisfactory.
Ultrasonography is safe and relatively inexpensive. No ionizing radiation is present, and damage to tissues has not been reported. The procedure permits continuation of suppressive therapy with thyroid hormone. Use of contrast material and patient preparation are unnecessary. Ultrasonography is of limited value adjacent to the trachea, is hard to interpret in the upper jugular region, and is not useful just behind the air-filled trachea or substernally.
NORMAL THYROID GLAND
The thyroid gland (Fig. 35-1) is characterized by homogeneous echoes, which give the gland a uniform ground-glass appearance. The surrounding muscles are of lower echogenicity. Medial to the thyroid lobes is the air-filled trachea, which does not transmit ultrasonic waves and is, therefore, poorly imaged. A calcified tracheal ring is represented anteriorly by dense echoes. The tubular carotid artery is echo free. Lateral and anterior to the carotid is the jugular vein, which can be identified when it is distended during a Valsalva maneuver. Behind the thyroid and anteromedial to the longus colli muscle is the esophagus, which can be identified as the patient swallows. The neurovascular bundle containing the inferior thyroid artery and recurrent laryngeal nerve may sometimes be identified, and blood vessels as small as 1 to 2 mm can occasionally be seen on the surface of the thyroid.
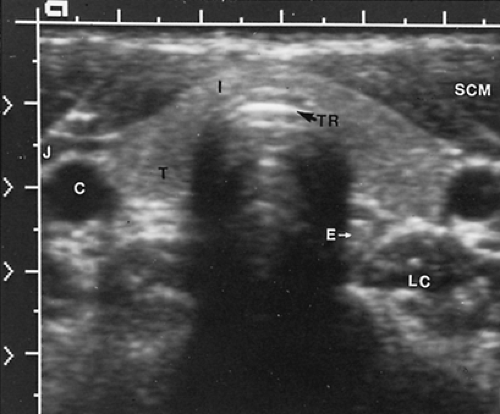 FIGURE 35-1. Sonogram of normal thyroid gland showing a transverse section of the lower anterior neck. Both lobes of the thyroid gland (T) are seen; they have a uniform, ground-glass appearance. The isthmus (I) is located anterior to the echo-dense tracheal ring (TR); behind that are artifactual reverberations of the sound waves. The carotid artery (C) and jugular veins (J) are found laterally. The sternocleidomastoid muscles (SCM) are anterior, and the longus colli muscles (LC) are posterior. The esophagus (E) is anteromedial to the left longus colli muscle. |
THYROID NODULE
Thyroid nodules distort the uniform echo pattern of the normal gland. Seventy-five percent of nodules are of lower echogenicity and 15% are of higher echogenicity than normal thyroid tissue, but this
characteristic has limited diagnostic value because most thyroid cancers are less echo-dense than normal tissue, and benign nodules may be more or less dense.4 The nodules may contain echo-dense deposits of calcium. Some nodules have a sonolucent rim called a halo (Fig. 35-2). Within small nodules, the echo texture tends to be uniform, but nodules larger than 2.5 cm usually have irregular, echo-free zones that represent cystic or hemorrhagic degeneration. These degenerative changes in a nodule may almost completely replace the solid structure, and careful examination in various planes is necessary to discern internal echoes that represent septa or small solid regions (Fig. 35-3). These complex “cystic” nodules are extremely common and must be differentiated from the rare true thyroid cyst, which is encountered in ˜1 in 500 to 1000 nodules4 (Fig. 35-4). A thyroid cyst is globular, smooth walled, and without internal echoes.
characteristic has limited diagnostic value because most thyroid cancers are less echo-dense than normal tissue, and benign nodules may be more or less dense.4 The nodules may contain echo-dense deposits of calcium. Some nodules have a sonolucent rim called a halo (Fig. 35-2). Within small nodules, the echo texture tends to be uniform, but nodules larger than 2.5 cm usually have irregular, echo-free zones that represent cystic or hemorrhagic degeneration. These degenerative changes in a nodule may almost completely replace the solid structure, and careful examination in various planes is necessary to discern internal echoes that represent septa or small solid regions (Fig. 35-3). These complex “cystic” nodules are extremely common and must be differentiated from the rare true thyroid cyst, which is encountered in ˜1 in 500 to 1000 nodules4 (Fig. 35-4). A thyroid cyst is globular, smooth walled, and without internal echoes.
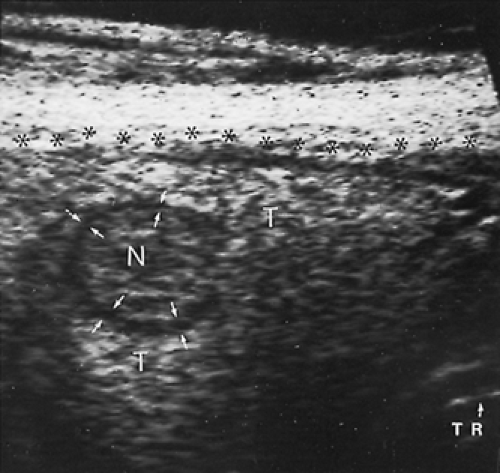 FIGURE 35-2. Sonogram of solid thyroid nodule showing the right thyroid lobe (T) of a patient who had a cold nodule (N). The nodule is of slightly lower echogenicity than the rest of the lobe and is surrounded by a halo (arrows) that is almost sonolucent. The lesion was a follicular adenoma. Asterisks indicate the anterior border of the thyroid lobe. (TR, a portion of a tracheal ring.) |
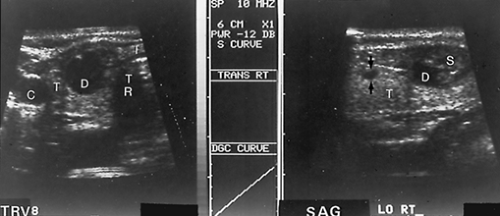 FIGURE 35-3. Sonogram of complex thyroid nodule. Sonograms in the transverse (TRV) and sagittal (SAG) planes of the right thyroid lobe (T) in a patient with a cold right thyroid nodule on radionuclide imaging. Previous aspiration yielded nondiagnostic debris. The sonograms show extensive degeneration (D) of the nodule. The lesion could easily be mistaken for a cyst in the transverse view. However, in the sagittal view, the solid component (S) is seen at the lower pole. This view was used as a guide to insert a needle into the solid component. The aspirate was consistent with a benign nodular thyroid. A second, low-echogenicity, 2 × 3 mm nonpalpable nodule higher in the right lobe in the sagittal view (arrows) suggests that this is a multinodular goiter. The increased acoustic shadowing behind the fluid-filled space in both views is caused by enhanced transmission of sound waves through fluid. The carotid artery (C), thyroid isthmus (I), and trachea (TR) are seen. The patient was given suppressive therapy after the fluid was aspirated. The solid component shrank, and the fluid did not reaccumulate. (From Blum M. Practical application of modern technology in thyroid evaluation. In: Van Middlesworth L, ed. The thyroid gland: practical clinical treatise. Chicago: Year Book Medical Publishers, 1986:58.) |
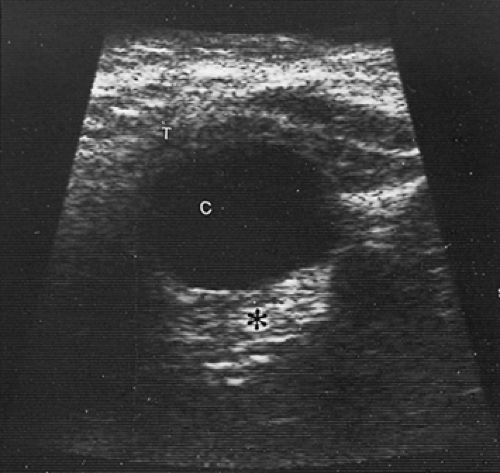 FIGURE 35-4. Sonogram showing a cyst (C) in the thyroid lobe (T). Dense echoes behind the cyst (*) signify enhanced transmission of the sound waves through the fluid-filled structure. No internal echoes are seen within the cyst space; it is globular in shape and has smooth walls.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|