SECRETION
NEURAL CONTROL
GH secretion is under neural control from the hypothalamus through at least two and possibly three hypophysiotropic factors: GH-releasing hormone (GHRH), somatostatin, and probably ghrelin (see following section). The GHRH neurons are located primarily in the arcuate and ventromedial nuclei, and somatostatin neurons are located primarily in the anterior periventricular area of the hypothalamus. GHRH and somatostatin release are controlled by a complex and incompletely understood neural network, involving α-adrenergic, dopaminergic, serotoninergic, cholinergic, and histaminergic inputs. In general, α-adrenergic, dopaminergic, serotoninergic, and cholinergic signals stimulate GH secretion. The limbic system plays an important role in GH secretion. A full discussion of the neural pathways regulating GH secretion is beyond the scope of this chapter. From a practical standpoint, it is important to know the physiologic stimuli leading to GH secretion, the principal pharmacologic agents used to test GH secretory capacity, and the peripheral feedback control of GH secretion.
GROWTH HORMONE–RELEASING HORMONE AND THE GROWTH HORMONE–RELEASING HORMONE RECEPTOR
GHRH is a 40- to 44-amino-acid peptide isolated first from pancreatic tumors that produced it ectopically,16,17 and subsequently from the hypothalamus (Fig. 12-8). Its gene, located on chromosome 20q, encodes a 108-amino-acid precursor from which GHRH is derived by proteolytic cleavage. It is expressed
in highest concentration in the hypothalamus, but also in other parts of the brain, in the gut, and in other tissues. The extrahy-pothalamic role of GHRH is largely unknown; it may act as a sleep inducer. GHRH is released from the median eminence into the pituitary portal system and is the principal stimulatory hypophysiotropic factor promoting GH secretion. (As mentioned earlier, GHRH is also important for the development of somatotrope cells15 and for GH synthesis.18) GHRH, on reaching the somatotropes, interacts with the GHRH-R, which is a seven transmembrane, Gsα-coupled receptor that signals through the cAMP and Ca2+-channel pathways (Fig. 12-9). Activation of these pathways effects GH release from secretory granules as well as GH gene transcription. The GHRH-R is expressed in a variety of tissues, but its biologic role in extrapituitary sites is unknown. GHRH is rapidly inactivated in plasma by an amino peptidase that cleaves the N-terminal dipeptide. Ectopic production of GHRH can occur in carcinoid and pancreatic islet tumors.
in highest concentration in the hypothalamus, but also in other parts of the brain, in the gut, and in other tissues. The extrahy-pothalamic role of GHRH is largely unknown; it may act as a sleep inducer. GHRH is released from the median eminence into the pituitary portal system and is the principal stimulatory hypophysiotropic factor promoting GH secretion. (As mentioned earlier, GHRH is also important for the development of somatotrope cells15 and for GH synthesis.18) GHRH, on reaching the somatotropes, interacts with the GHRH-R, which is a seven transmembrane, Gsα-coupled receptor that signals through the cAMP and Ca2+-channel pathways (Fig. 12-9). Activation of these pathways effects GH release from secretory granules as well as GH gene transcription. The GHRH-R is expressed in a variety of tissues, but its biologic role in extrapituitary sites is unknown. GHRH is rapidly inactivated in plasma by an amino peptidase that cleaves the N-terminal dipeptide. Ectopic production of GHRH can occur in carcinoid and pancreatic islet tumors.
 FIGURE 12-8. Amino-acid sequence of growth hormone–releasing hormone (GHRH) 1-40 (top) and 1-44 (bottom). GHRH 1-44 has four additional amino acids at the C-terminal end of the molecule and is amidated. |
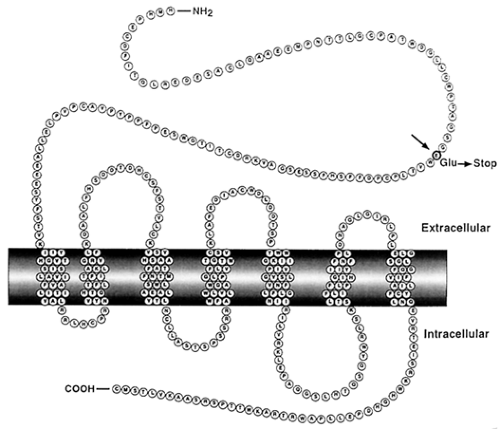 FIGURE 12-9. Primary structure of the growth hormone–releasing hormone (GHRH) receptor, showing the seven transmembrane helices. The location of a nonsense mutation responsible for familial GHRH-resistant dwarfism is also shown (see text on congenital growth hormone deficiency). (From Maheshwari HG, Silverman BL, Dupuis J, Baumann G. Phenotype and genetic analysis of a syndrome caused by an inactivating mutation in the growth hormone releasing hormone receptor: dwarfism of Sindh. J Clin Endocrinol Metab 1998; 83:4065.) |
SOMATOSTATIN AND SOMATOSTATIN RECEPTORS
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


