PITUITARY TUMORS
CLASSIFICATION
The classic histologic designation of adenomas as chromophobic, eosinophilic, or basophilic on the basis of light microscopy is now obsolete and has been replaced by a system that classifies adenomas according to the hormones they secrete1 (see Chap. 11). The term chromophobe adenoma has been replaced by terminology that designates two types of nonsecreting tumors: the oncocytoma, which is thought to be a neoplasm with transformed epithelial cells without endocrine potential, and the null cell adenoma, which may have an as yet unidentified secretory product.2
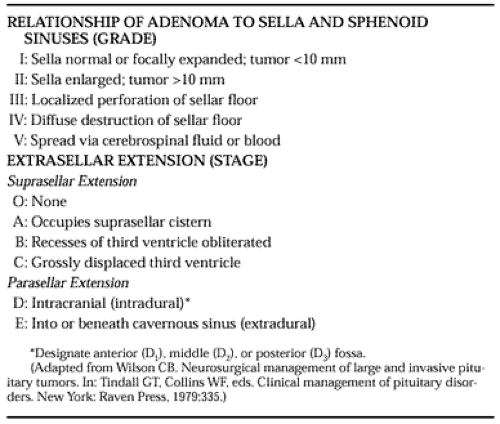
Patients with tumors of the pituitary present for treatment either because of endocrinopathy or because of local mass effects. Classification according to the degree of sellar destruction (grade) and extrasellar extension (stage) can assist the physician in determining the surgical prognosis3 (Table 23-1).
 |
RADIOLOGIC EVALUATION
Before MRI scanning reached its present level of sophistication, the diagnosis of a pituitary tumor was based on thin-section polytomography of the sella, pneumoencephalography, computed tomography (CT) scanning, and bilateral carotid angiography. MRI scanning with and without gadolinium enhancement, with magnified images obtained in the axial, coronal, and sagittal planes, has made pneumoencephalography, CT scanning, and polytomography obsolete because it can more accurately diagnose pituitary adenomas in most cases (see Chap. 20). An MRI diagnosis of adenoma is based on the fact that both normal pituitary gland tissue and the adjacent cavernous sinuses enhance at a different time after the administration of intravenous paramagnetic contrast material than does an adenoma, which often enhances poorly, and usually late.4 The timing of imaging is important. Most radiologists recommend imaging as soon as possible after the administration of the contrast. Other criteria suggestive of adenoma include a convex upper border of the pituitary gland (seen, however, in 2% of normal glands); increased height of the gland (>7 mm); lateral deviation of the pituitary stalk; and a focal area of altered attenuation relative to the normal gland, on either contrast or noncontrast studies. Usually, precise delineation between tumor and other important structures in the area can be accomplished (Fig. 23-1).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


