Chapter 46 Pancreatic Cancer
Managing pancreatic adenocarcinoma presents significant challenges. The natural history of the disease is characterized by spread to regional lymphatics, liver, and peritoneal surfaces; and most patients have either clinical or subclinical dissemination to these sites at diagnosis. At presentation, the outcome appears to be determined primarily by the extent of evident disease, resectability, and performance status. Patients with resectable tumors have historically been thought to represent 15% to 20% of those with pancreatic cancer. However, recent Surveillance, Epidemiology, and End Results (SEER) data analyses suggest that in the United States the frequency of potentially resectable disease may be closer to 10% to 12%.1
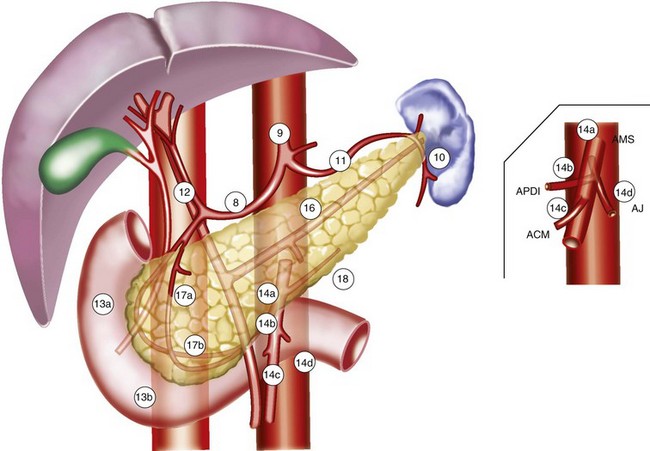
Most (75% to 80%) pancreatic adenocarcinomas present in the head, neck, and/or uncinate process (periampullary region), and results from these presentations provide the dataset from which clinical management decisions are most commonly made. The dataset for management decisions regarding presentations in the distal pancreatic body and tail is much less robust. The anatomic relationships of the pancreas are illustrated in Figure 46-1.
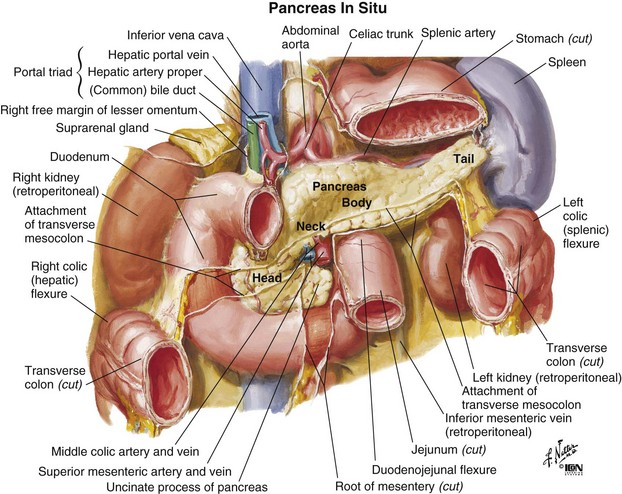
Figure 46-1 Anatomy of the pancreas.
From Netter FH: Atlas of Human Anatomy. West Caldwell, NJ, 1992, CIBA-GEIGY Corporation, plate 279.
Epidemiology And Etiology
Epidemiology
In 2010 there were an estimated 43,140 new cases of pancreatic carcinoma in the United States, with slightly more cases in women than in men.2 In the same year the number of deaths due to carcinoma of the pancreas was estimated to be 36,800. It was anticipated that carcinoma of the pancreas would be the 10th most frequently diagnosed new cancer in men and women, but the 4th leading cause of cancer death (after lung, prostate, and colorectal cancer in men and lung, breast, and colorectal cancer in women). Internationally, incidence rates are highest in Western and industrialized countries.
Most patients with pancreatic cancer present with advanced disease. Incidence rates increase with age, and most cases occur in patients older than 60 years of age. Approximately 68% of cases will be diagnosed in patients 65 years of age or older. In the absence of overt metastatic disease, patients undergoing pancreatic resection have a clear survival advantage as compared with patients not undergoing resection. The 1-, 2-, and 3-year overall survival (OS) rates for patients undergoing resection as compared with those not undergoing resection are 48% versus 23%, 24% versus 9%, and 17% versus 6%, respectively.3
Etiology
Pancreatic cancer is clearly associated with cigarette smoking, diet (higher risk with higher percentages of fat and meat in the diet), obesity,4 chronic diabetes mellitus, and chronic pancreatitis. Of these, the strongest association is with cigarette smoking. There is also an occupational association with the manufacture of 2-naphthylamine and benzidine and with those working with gasoline derivatives.5 Although coffee consumption has sometimes been implicated in the occurrence of carcinoma of the pancreas, a review failed to confirm this association.6
There is an increased risk of developing pancreatic cancer, as well as other intra-abdominal malignancies, after radiation therapy (RT) to the abdomen for management of testicular malignancy, either seminoma or nonseminoma (the observed to expected frequency is 2.30).7 The risk is noted as early as 10 years after management and continues to increase with time.
An important development in our understanding of the etiology of pancreatic cancer is the recognition of familial pancreatic cancer.8 Familial pancreatic cancer may occur in the absence of a recognizable clinical syndrome, and as many as 10% of pancreatic cancers may be familial. Data from the National Familial Pancreas Tumor Registry have shown that the risk of cancer is 18-fold greater in first-degree relatives of familial pancreatic cancer cases (at least two first-degree relatives with pancreatic cancer in the family) than it is in first-degree relatives of sporadic pancreatic cancer cases (families in which there has been only one member with pancreatic cancer).9 In addition, there are associations with other known syndromes such as the familial breast, ovarian, pancreas cancer syndrome associated with BRCA2, the familial pancreas cancer syndrome associated with CDKN2A abnormalities, the Peutz-Jeghers polyposis gastrointestinal malignancy syndrome associated with mismatched repair genes, LKB1/STK11, and the hereditary nonpolyposis colon cancer (HNPCC) syndrome. Current understanding of familial pancreatic cancer has been reviewed by Shi and associates10 and is regularly updated at the webpage of the Johns Hopkins National Familial Pancreatic Tumor registry (pathology.jhu.edu/pancreas/PartNFPTR.php).11
Prevention And Early Detection
Although the just described associations might suggest the identification of a patient population suitable for screening, so far no simple, cost-effective test for the disease has been successful in establishing early diagnosis even in relatively high-risk groups.12 Potential imaging modalities for screening and early detection include computed tomography (CT), magnetic resonance imaging (MRI), and endoscopic ultrasonography (EUS). For early detection, EUS may be the imaging modality of choice because it detects smaller pancreatic lesions than those detected with thin-section, dual-phase spiral CT. The accuracy of diagnosis of pancreatic cancer in patients with pancreatic masses suspected of having cancer is close to 100% for EUS and about 92% for dual-phase CT.13 When combined with fine-needle aspiration (FNA), EUS can provide a cytologic diagnosis of lesions as small as 2 to 5 mm not visualized by CT, ultrasonography, or MRI. Endoscopic retrograde cholangiopancreatography (ERCP) is less likely to detect small tumors, is a relatively more invasive screening test owing to the risk of developing pancreatitis (5% to 10%), and may be useful for detailed characterization of ductal abnormalities. Unfortunately, recent efforts at applying these methodologies appear to have been unrewarding, suggesting that, at present, screening even in identified, high-risk populations may not be appropriate.14–15 However, it remains possible that screening of individuals from the highest-risk kindreds (those with three or more first-degree relatives with pancreatic cancer), based on experience at the Johns Hopkins Hospital,16,17 might be useful.
Presently, there is no routinely available blood test that may be used as a screening tool for pancreatic cancer. Although serum carbohydrate antigen 19-9 (CA19-9) is a tumor-associated antigen that is frequently elevated in patients with pancreatic adenocarcinoma,18 it may also be elevated in biliary tract malignancies, some colon cancers, and non–cancer-related conditions such as pancreatitis, cholangitis, poorly controlled diabetes, and biliary obstruction due to benign causes (stones, strictures). Moreover, patients genetically lacking Lewis antigens may be incapable of producing CA 19-9. Consequently, CA 19-9 is better used to help monitor therapeutic response when elevated secondary to tumor in patients with histologically proven pancreatic cancer.19,20,21
Biomarkers for early detection targeting are in development and include DNA-, RNA-, and protein-based approaches. DNA-based techniques aim to detect cancer-specific DNA alterations and methylation changes.22 Analysis of pancreatic juice or fine-needle aspirates may identify genes overexpressed at the RNA level in pancreatic cancers compared with normal pancreas.23 Protein-based markers may also be overexpressed in patients with pancreatic cancer compared with patients with other pancreatic diseases.24
Biologic Characteristics And Molecular Biology
A number of studies have looked at DNA content and proliferative index in patients with pancreatic cancer. Bottger and associates25 studied DNA content, tumor size, lymph node status, tumor stage, nuclear grade, and type of resection on outcomes in a series of 41 patients with adenocarcinoma of the pancreas. They observed that in univariate analysis these factors had a significant (p <.05) association with outcome. However, in multivariate analysis the most important predictors of outcome were the operative procedure (whether the tumor was resected to histologically negative margins) and the DNA content (whether the patient’s tumor was tetraploid, having unfavorable prognostic implications). Similarly, Jorba and colleagues26 found that among 73 patients undergoing pancreaticoduodenectomy for periampullary malignancies, 74% were diploid and 26% were aneuploid. In univariate analysis there was a strong correlation between diploid status and long-term survival, with diploid cancer patients having a median survival of 30.1 months and aneuploid cancer patients having a median survival of 16 months. However, when tumor site (duodenum and ampulla vs. bile duct and pancreas) and tumor size were taken into consideration, the effect of ploidy no longer produced a significant difference.
As summarized by Hruban and colleagues,27 cancer of the pancreas can now be viewed as a disease of acquired and inherited mutations involving a number of cancer-related genes. There are three types of such genes: tumor suppressor genes, oncogenes, and DNA mismatch repair genes. Tumor suppressor genes function to restrain cell proliferation. Oncogenes possess transforming properties when activated by mutation or amputation. DNA mismatch repair genes encode for proteins that correct errors that normally occur during DNA replication. All three types of potentially cancer-causing genes have been implicated in pancreatic cancer.
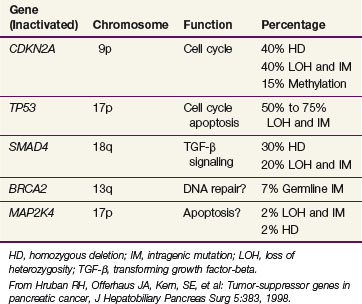
A number of suppressor genes have been found to play a role in the development of pancreatic cancer. Table 46-1 provides a summary of the tumor suppressor genes in pancreatic cancer.27 The CDKN2A tumor suppressor gene on chromosome 9p is inactivated in approximately 95% of pancreatic cancers. The mechanism by which CDKN2A inactivation promotes cell cycle progression is shown in
web-only Figure 46-1 on the Expert Consult website
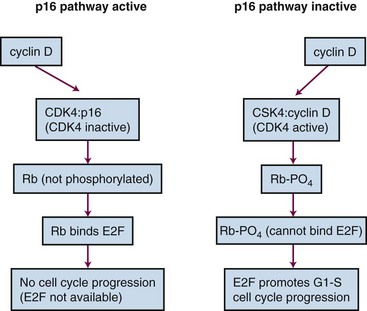
Web-Only Figure 46-1 Inactivation of CDKN2A promotes cell cycle progression.
From Tascilar M, Skinner HG, Rosty C, et al: The SMAD4 protein and prognosis of pancreatic ductal adenocarcinoma. Clin Cancer Res 7:4115, 2001.
The TP53 gene located on chromosome 17p is inactivated in 50% to 70% of pancreatic cancers. The SMAD4 gene on chromosome 18q is inactivated in approximately 50% of pancreatic cancers. It has been found to be of prognostic significance, with SMAD4-positive patients having improved survival over SMAD4-negative patients. Moreover, SMAD4 positivity retains its prognostic significance in multivariate analysis adjusting for tumor size, lymph node involvement, margin status, and histologic differentiation.28 The BRCA2 gene is inactivated in 70% of pancreatic cancers. BRCA2 is noteworthy because it represents mutation in the inherited germline in some cases. Additionally, BRCA2 has been confirmed as the most common inherited genetic alteration associated with pancreatic cancer.29
Finally, abnormalities in DNA mismatch repair genes have been noted. A specific molecular phenotype called microsatellite instability, also identified in the HNPCC syndrome of colon cancer, has been found in 4% of pancreatic cancers and is associated with a unique morphologic appearance, the presence of wild-type (normal) KRAS, diploidy, and improved prognosis.30
These molecular abnormalities have several applications. They may be used to define the precursors of infiltrating adenocarcinoma of the pancreas or help characterize histologically ambiguous lesions. Moreover, they have the potential to form the basis for new screening tests for pancreatic neoplasia and, subsequently, may serve as important epidemiologic tools.27
Just as specific genetic abnormalities have been associated with pancreatic cancer, karyotyping studies by Griffin and colleagues31,32 have shown consistent losses of chromosomes 18, 13, 12, 17, and 6. This correlates well with the loss of the SMAD4 suppressor gene, which is known to reside on chromosome 18, and the loss of the tumor suppressor gene TP53, which is known to reside on chromosome 17.
In recognition of an evolving understanding of the role of genetics and familial clustering of pancreatic adenocarcinoma, the Johns Hopkins Familial Pancreatic Tumor Registry was established in 1994 and has produced a number of important observations regarding the risk of pancreatic cancer in families with two or more first-degree relatives and genetic patterns in these families. The most recent update of the Johns Hopkins registry was in 2009, and the website can be viewed online (see earlier discussion). First-degree relatives from kindreds in which there are two first-degree relatives with pancreatic cancer may have as much as a 9-fold higher risk of developing pancreatic cancer than a member of the general population. If there are three or more first-degree relatives, this risk increases up to 32-fold. The risk relates to blood-line relatives and does not include spouses. There are now multiple registries for familial pancreatic cancer, and there has been a suggestion for developing an international registry to combine these efforts.33
Pathology And Pathways Of Spread
Pathology
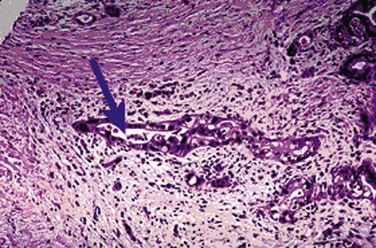
Infiltrating ductal adenocarcinomas are the most common histologic type of malignant tumors of the exocrine pancreas, as shown in Figure 46-2. These malignant epithelial neoplasms show glandular or ductal differentiation, with most arising in the periampullary region of the pancreas.34 Although ductal adenocarcinoma is the most common primary malignancy of the pancreas, accounting for approximately 75% of all primary nonendocrine cancers in this organ, there are a number of other important epithelial malignancies arising in the pancreas that should be recognized because of their variant presentations and prognostic implications.35 Recent reports have nicely summarized the progression of pancreatic intraepithelial neoplasia to invasive ductal carcinoma and also described the molecular and prognostic correlates associated with less common pancreatic tumors.36,37
Acinar cell carcinoma is also a rare histology in which 20% of cases may be associated with subcutaneous fat necrosis, a rash similar to erythema nodosum, peripheral eosinophilia, and polyarthralgias. These associated phenomena are a result of release of large amounts of lipase by the tumor.38 These tumors typically present with large size and average dimension of 11 cm and occur in the head, body, and tail of the pancreas with frequencies of 60%, 30%, and 10%, respectively. Survival is not significantly superior to that seen with standard adenocarcinoma of the pancreas. Those patients presenting with large amounts of lipase production may have a less than average prognosis.
The primary cystic, nonendocrine epithelial tumors are another type of pancreatic neoplasm. Only 5% to 15% of pancreatic cystic lesions are actually neoplastic, with the remaining non-neoplastic lesions including pseudocysts, congenital cysts, and retention cysts. The cystic neoplasms of the pancreas include serous and mucinous neoplasms. Most serous cystic neoplasms are serous cystadenomas, also known as microcystic adenomas and glycogen-rich cystadenomas. They occur more commonly in women, with average age at presentation in the seventh decade.39 These lesions may be large, and patients with von Hippel-Lindau syndrome (familial cancer syndrome associated with clear cell renal cancer, cerebellar and spinal hemangioblastomas, pancreatic islet cell cancers, and other tumors) may be predisposed to develop pancreatic serous cystadenomas. Most serous cystic neoplasms of the pancreas are benign.
In contrast, mucinous cystic neoplasms are more frequently malignant. These are also more common in women and are typically diagnosed in the fifth decade of life. Histologically, these lesions contain a mucin-positive, cloudy fluid and do not communicate with the main pancreatic duct.40 Microscopic analysis reveals three types of mucinous cystic neoplasms: mucinous cystadenomas, borderline mucinous cystic neoplasms, and mucinous cystadenocarcinoma. It is generally thought that mucinous cystadenomas and borderline cystic neoplasms have the potential for progressing to overt malignancy and should be completely resected. Interestingly, mucinous cystadenocarcinomas are associated with a better prognosis than typical adenocarcinoma of the pancreas, with roughly 50% of patients surviving 5 years.
Intraductal papillary mucinous neoplasms communicate with the main pancreatic duct system and are typically diagnosed in the seventh decade. They are associated with a good prognosis compared with more typical pancreatic malignancies.41 A more aggressive variant is the papillary mucinous carcinoma in which the histology displays significant cytologic and architectural atypia and/or overt invasion.
It has been well known that a precursor histology of intraepithelial neoplasia (IN) can be described in sites such as colon, cervix, and prostate. The precursor histology for pancreatic adenocarcinoma (PanIN) has also been well described.42 These lesions have been named PanIN-1A and 1B, PanIN-2, and PanIN-3. They are often seen in association with invasive adenocarcinoma and have occasionally been observed to progress into invasive adenocarcinoma.
Pathways of Spread
The pancreas is a retroperitoneal organ that lies in close anatomic relationship to the stomach, duodenum, jejunum, kidneys, spleen, celiac trunk, superior mesenteric artery and vein, common bile duct, and portal vein (see Fig. 46-1). The main pancreatic duct is known as the duct of Wirsung, and the accessory pancreatic duct is known as the duct of Santorini. At the time of diagnosis, more than 85% of pancreas tumors will have extended into adjacent organs, lymph nodes, fat, or soft tissue, allowing early metastasis to regional and distant lymph nodes.43
Patterns of involvement in the regional lymphatics have long been well recognized. Frequently involved nodal sites include the posterior pancreaticoduodenum, superior pancreatic head, inferior pancreatic head, superior pancreatic body, and porta hepatis.44,45 There is also a relationship between para-aortic lymph node involvement and involvement of posterior pancreaticoduodenal nodes by direct interlymphatic communication46 (Fig. 46-3). Venous drainage of the pancreas is to the liver via the portal vein.
Patterns of failure after resection have been described, with local recurrence, peritoneal relapse, and hepatic metastases occurring in 50%, 42%, and 62% of patients, respectively.47,48–50 Although it is likely that the peripancreatic burden of disease has multiple direct lymphatic pathways to hepatic tissues, hepatic involvement has been taken as a sign of systemic metastasis. The lung is the most frequently involved extra-abdominal organ.43
Recent reports confirm that these patterns of failure have not changed appreciably over time and also emphasize the effect of the retroperitoneal margin, poor differentiation, and lymph node involvement in determining relapse risk, especially locally.51,52 In addition, rapid autopsy results from Johns Hopkins Hospital studies indicate that local recurrence may be associated with alterations in SMAD4 and that local recurrence may be the cause of death in up to 30% of patients with overt metastatic disease.53
Clinical Manifestations, Patient Evaluation, And Staging
Initial laboratory results may show elevated serum bilirubin, alkaline phosphatase, and gamma glutamyl transpeptidase levels. In addition, the hepatic aminotransferases may be increased. Although CA19-9 has not proved useful as a marker for screening of pancreatic cancer, it has been used as a test to assess prognosis and/or follow patients postoperatively as well as to guide prognosis and response to other treatment when known to be previously elevated in association with a proven pancreatic malignancy.54,55 The value of CA19-9 was confirmed prospectively in analysis of data from the Radiation Therapy Oncology Group (RTOG) 97-04 trial, which showed on multivariate analyses that the postoperative CA19-9 level is a highly significant predictor of overall survival in patients with resected pancreatic cancer.21 Some early data suggest that monitoring levels of KRAS after treatment may possibly give clues as to tumor response in patients treated with gefitinib and chemoradiation, but this has not been proved.56
Patient Evaluation
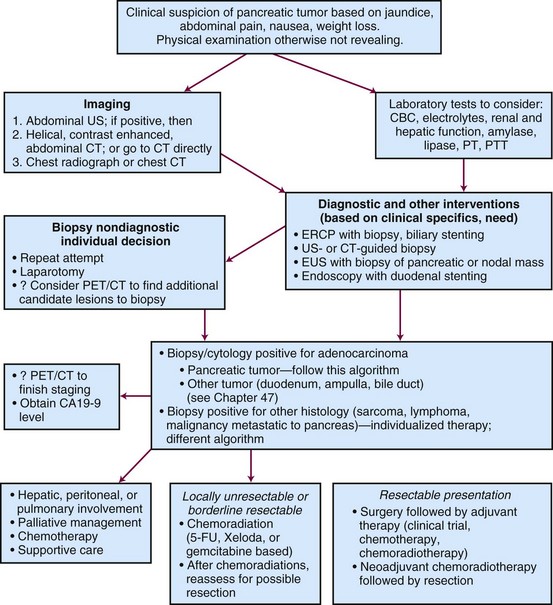
Assessment is guided by the patient’s presenting symptoms, findings on history and physical examination, and initial laboratory results (Fig. 46-4). Ultrasonography, CT, and ERCP are often included in the evaluation of patients with obstructive jaundice. With current spiral CT techniques combined with enhancement after oral and intravenous administration of contrast, pancreatic masses, pancreatic duct dilatation, local invasion, liver metastases, and vascular invasion of the great vessels are readily identified. EUS has improved staging of pancreatic cancer. It is especially effective in detecting vascular invasion of pancreatic cancer when CT is equivocal, which is imperative in determining resectability.57 ERCP is frequently used to obtain biopsy specimens, decompress the biliary tree, and localize the source of obstruction. Biliary obstruction can also be relieved by percutaneous and transhepatic cholangiography. Visceral angiography is selectively used based on concern regarding vascular invasion leading to unresectability. PET may be useful in identifying otherwise occult metastases. A study of 82 patients staged with either CT alone or PET/CT showed that the addition of PET increased sensitivity for the detection of distant metastases and would have changed management in 11% of the patients.58 Laparoscopy is used in some institutions as a prelude to exploration and has been found to increase the detection of intraperitoneal metastases in patients with locally advanced pancreatic cancer. It appears that a tissue diagnosis by FNA before laparotomy is not necessary.59
Staging
The seventh edition of the American Joint Committee on Cancer (AJCC) staging system for pancreatic cancer is shown in Table 46-2. There were no changes between the AJCC sixth and seventh editions, except that the seventh edition now includes neuroendocrine tumors. Treatment and prognosis are defined by resectability (T < T4) and presence of distant metastatic disease, which most commonly involves the liver, peritoneum, or both.60
TABLE 46-2 American Joint Committee on Cancer TNM Staging for Pancreas Cancer
| Primary Tumor (T) | |
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor limited to the pancreas ≤2 cm in greatest dimension |
| T2 | Tumor limited to the pancreas >2 cm in greatest dimension |
| T3 | Tumor extends beyond the pancreas but without involvement of the celiac axis or the superior mesenteric artery |
| T4 | Tumor involves the celiac axis or the superior mesenteric artery (unresectable primary tumor) |
| Regional Lymph Nodes (N) | |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Regional lymph node metastasis |
| Distant Metastasis (M) | |
| MX | Distant metastasis cannot be assessed |
| M0 | No distant metastasis |
| M1 | Distant metastasis |
From Edge SB, Byrd DR, Compton C, et al, editors: AJCC Cancer Staging Manual, ed 7, New York, 2010, Springer.
Pancreatic tumors staged as T1, T2, or T3 are generally considered to be resectable. Unresectable pancreatic tumors are those in which the tumor cannot be separated from the adjacent large arterial structures (celiac axis or superior mesenteric artery). The extent of resection also carries prognostic significance. A patient who has undergone an R0 complete resection with negative margins will have a better prognosis compared with a patient who has undergone an R1 or R2 resection with microscopic (R) or grossly positive margins (R2). Furthermore, recent data suggest that margins greater than 1.5 mm are needed to optimize locoregional control, and the extent of clear margins in R0 resections may potentially be used to estimate risk of locoregional failure.61 Borderline resectable tumors, which are at high risk for a margin-positive resection, are discussed later in this chapter.
Primary Therapy
Surgery
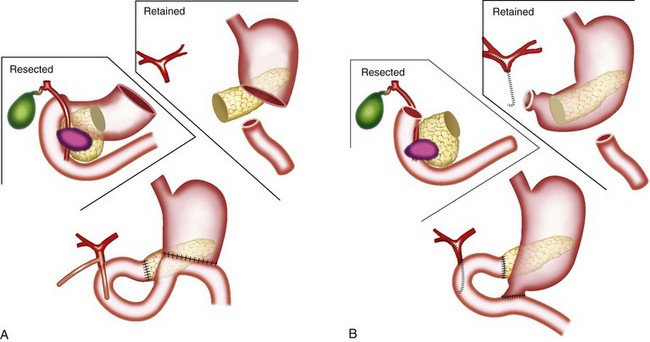
The classic operation for resection of a carcinoma of the head of the pancreas is a pancreaticoduodenectomy, also known as a Whipple procedure. In this operation the gallbladder, common bile duct, second through fourth portions of the duodenum, and the head of the pancreas are resected along with the postpyloric duodenum (pylorus-preserving pancreaticoduodenectomy) or the resection is continued proximally to include the distal stomach (classic pancreaticoduodenectomy). The regional lymph nodes are also resected. It appears well established that the pylorus-preserving pancreaticoduodenectomy improves gastrointestinal function without compromise of oncologic management.62–64 Figure 46-5 illustrates these two variants of surgical resection.65 Within the past two decades, the mortality of this operation has declined from approximately 20% to between 1% and 3% in major centers.66–68 (A video of this operation may be observed at www.orlive.com/umm/videos/whipple-procedure-for-pancreatic-cancer.)
web-only Figure 46-2, available on the Expert Consult website
.69 As illustrated, gastrointestinal reconstruction after pancreaticoduodenectomy requires enteric, biliary, and pancreatic anastomoses. Although postoperative mortality is less than 3% at high-volume centers, the morbidity of pancreaticoduodenectomy remains high, with pancreatic leak and infection, delayed gastric emptying, and pancreatic fistula among the most common complications.70 Based on large-volume, single-institution experience the dramatic improvements in postoperative morbidity and mortality reported in the 1990s have not shown further improvement.71
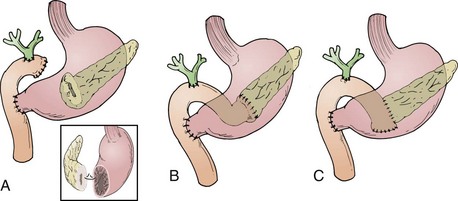
Web-Only Figure 46-2 A, Pancreaticogastrostomy. B, End-to-end pancreaticojejunostomy. C, End-to-side pancreaticojejunostomy. The inset details the location of the posterior gastrostomy.
From Yeo CJ, Cameron JL, Maher MM, et al: A prospective randomized trial of pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy. Ann Surg 222:580, 1995.
Prognostic Factors Associated with Results of Surgical Resection
Michelassi and colleagues72 reported on their experience with 647 consecutive patients between 1946 and 1987 with tumors of the duodenum, ampulla, head of the pancreas, and distal common bile duct, including patients with resectable and nonresectable disease. The resectability rate varied from 16.5% for pancreatic adenocarcinoma to 89.3% for ampullary tumors. Among these 647 patients, there were 133 resections. Their data clearly show the importance of resection for any type of tumor presentation in the periampullary area with respect to 5-year survival. Evaluating only those patients with adenocarcinoma who underwent a curative intent resection and survived the perioperative period (n = 97), the following factors did not affect survival: tumor size, tumor differentiation, the presence of lymphovascular invasion, capillary invasion, perineural microinvasion, lymph node status, or type of procedure (pancreaticoduodenectomy vs. total pancreatectomy). The authors analyzed relapse data and found that based on autopsy experience 29.4% of patients died with local recurrence alone, 23.5% died with distant metastasis alone, and 47.1% had both local and distant relapses.
Yeo and colleagues73 have published two important papers that summarize and describe the anticipated patient experience after surgery for periampullary malignancy. In their series of 650 consecutive pancreaticoduodenectomies in the 1990s, there were 443 patients who underwent resection for periampullary malignancy. Their data convincingly show the improved survival seen for resected duodenal and ampullary tumor as opposed to resected pancreatic and distal common bile duct tumors. Moreover, in multivariate analysis, factors associated with improved, postresection survival are the absence of intraoperative blood loss greater than 700 mL, tumor site (with duodenum and ampullary being better than bile duct and pancreas), tumor diameter of less than 3 cm as opposed to 3 cm or more, histologically negative margins, histologically negative nodes, and having a well-differentiated tumor as opposed to a moderately or poorly differentiated tumor. Reoperation for complication was also significantly associated with decreased survival. Yeo and associates74 further analyzed factors associated with long-term survival in 242 patients who underwent surgery between April 1990 and May 1992. They found that negative nodal involvement, tumor differentiation, and resected margin status were all important prognostic factors for periampullary tumors. A more recent update from the same institution has also added extent of lymph node involvement to these previously identified risk factors.75
The prognostic importance of histologic differentiation, nodal involvement, and tumor size (for patients with pancreatic adenocarcinoma) have also been demonstrated by Geer and Brennan.76 The difference in survival at 36 months for well-differentiated tumors versus poorly differentiated tumors is roughly 50% and 10%, respectively. Less extreme but still highly significant differences are seen when comparing node-negative survivors versus node-positive survivors. At 36 months the survivals were approximately 35% and 10%, respectively. In tumors smaller than or larger than 2.5 cm, the survival differences were 40% and 20%, respectively. This group has developed a nomogram based on data from 555 patients to predict outcome at 1, 2, or 3 years.77 The factors correlating with survival in their multivariate analysis are shown in Table 46-3. This nomogram can be accessed at the web page of the Memorial Sloan-Kettering Cancer Center (www.mskcc.org).
TABLE 46-3 Factors Correlating with Survival in Multivariate Analysis
| Factor | p Value |
|---|---|
| Maximum tumor dimension | .001 |
| Number of nodes positive | .001 |
| Splenectomy required | .001 |
| Differentiation | .002 |
| Tumor located in head versus other pancreatic site | .006 |
| Posterior margin status | .049 |
Data from Brennan MF, Kattan M, Klimstra D, Conlon K: Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas, Ann Surg 240: 293, 2004
Although size has prognostic importance in pancreatic cancer, small size does not necessarily equate with a low-risk lesion, as demonstrated by Manabe and colleagues in 1988.78 This observation has subsequently been confirmed in more contemporaneous series.79,80
Patterns of Failure After Surgical Resection
Tepper and colleagues47 reported on 145 patients managed at the Massachusetts General Hospital from 1963 to 1973. Of these patients, only 31 underwent radical surgery, with 5 operative deaths, leaving 26 patients for further analysis. Among these 26 patients, 50% had either pathologically proven local recurrence or clinical evidence of local recurrence at the time of death from disease. In 5 patients, local status was unknown at the time of death. Four patients died of distant metastases without evidence of local recurrence.
Griffin and associates48 did a more extensive analysis of patterns of failure after curative resection for pancreatic carcinoma. This analysis was on 36 patients undergoing resection with curative intent at the University of Kansas between 1977 and 1987. The 2- and 5-year survivals among these patients were 32% and 17%, respectively. The median survival was 11.5 months. Of all the patients who had failure, 100% had a component of failure within the intra-abdominal cavity. Seventy-three percent had a component of local failure, 42% had a component of peritoneal failure, and 62% had a component of hepatic failure. Extra-abdominal metastases were documented in only 27% of patients and never as the sole site of disease.
Foo and colleagues81 described the outcome of 29 patients treated with RT after curative surgery for pancreatic cancer at the Mayo Clinic between 1974 and 1986. Their data suggested a significant increase in survival when adjuvant chemoradiation was combined with surgery compared with surgery alone. Eighty-three percent of patients eventually experienced relapse. Among patients receiving chemotherapy and RT, the chemotherapy was 5-fluorouracil (5-FU) and the RT usually consisted of doses between 45 and 54 Gy. In contrast to the studies by Tepper and Griffin and their colleagues,47,48 as a result of adjuvant chemoradiation there was only a 7% rate of local failure. Liver failure and peritoneal seeding remained high at 43%, with 61% of patients having a component of either liver or peritoneal relapse.
Kayahara and associates49 reported on 45 patients undergoing curative resection of carcinoma of the head of pancreas between 1974 and 1991. Of these patients, 30 eventually experienced relapse. Documented at autopsy, patterns of failure included local recurrence in 80%, hepatic metastases in 66%, peritoneal dissemination in 53%, and lymph node relapse in 47%.
Finally, Willett and colleagues82 analyzed patterns of failure after pancreaticoduodenectomy for periampullary carcinoma in 41 patients (surgery alone in 29 patients; adjuvant postoperative RT in 12 patients). They observed excellent local control of 88% with T stages of in-situ disease, T1, or T2 stage compared with 44% for T3 or T4 local stages. Patients with lymph node positivity had a local control rate of 47%, whereas patients with negative lymph nodes had a local control rate of 87%. Moderately differentiated tumors had a local control rate of 81% as compared with patients with poorly differentiated tumors with a 0% 5-year local control rate (3 patients). In the 17 surgery-alone patients who had high-risk features, as defined by the authors (tumor invading the pancreas, poorly differentiated, involved nodes, and positive resection margins), the 5-year local control and OS rates were 50% and 38%, respectively. For the 12 high-risk patients who received postoperative irradiation alone or plus concurrent 5-FU there was a trend toward improvement in 5-year local control (83% vs. 50%) and 5-year OS (51% vs. 38%) rates, but this did not reach statistical significance in view of small patient numbers and the rate of distant metastasis.
Adjuvant Chemotherapy and Irradiation after Resection, Randomized Data
In 1974, the Gastrointestinal Tumor Study Group (GITSG) undertook a prospective, randomized trial of adjuvant 5-FU–based chemoradiation compared with no adjuvant treatment.83,84 This was a well-designed trial that attempted to recruit patients with histologically negative margins of resection between 4 and 10 weeks postoperatively. However, only 49 patients were randomized into the study over an 8-year interval; moreover, 5 withdrew without being treated. The external beam irradiation (EBRT) was given as two courses of 20 Gy in 10 fractions, each with a planned 2-week rest. Treatment fields did not exceed 20 × 20 cm and were given anterior-posterior/posterior-anterior. Shaping of fields was optional, and 5-FU chemotherapy was given on the first 3 days of each half of the RT at a dose of 500 mg/m2 as an IV bolus. Thirty-five percent of patients had tumor confined to the pancreas, 37% had contiguous invasion resected to clear margins, and 28% had nodal involvement.
Results showed that patients treated with combined chemoradiation had improved survival (p = .03) compared with patients treated with surgery alone, with a median survival in the treatment group of 20 months versus 11 months in the control arm (Table 46-4). Two-year OS was 42% versus 15%, respectively, and 5-year OS was 19% versus 5%. Prognostic factors including age, sex, type of resection, degree of cellular differentiation, initial performance status, location of tumor, and extent of tumor were evaluated. Performance status and extent of tumor were the only independently significant prognostic variables. The study was terminated prematurely because of poor accrual in spite of the long period of time during which it was open.
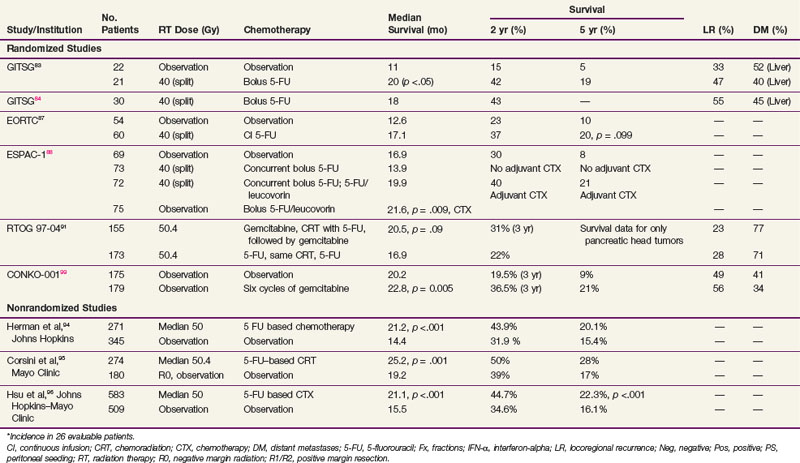
TABLE 46-4 Adjuvant Radiation Therapy and Chemotherapy for Resected Ductal Adenocarcinoma of the Pancreas, Selected Series
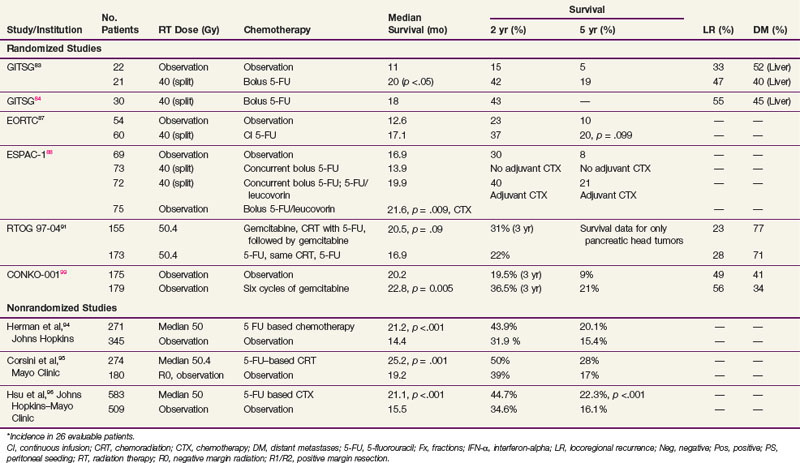
In an effort to address concerns due to poor accrual, the GITSG registered an additional 30 patients in a nonrandomized fashion to receive the same adjuvant therapy. Results in these 30 patients recapitulated the results of the treatment arm in the previous randomized study.84 It was of interest to note that, although the treatment produced relatively little toxicity, the local recurrence rate was between 30% and 50% in all patients regardless of whether they received adjuvant treatment and the incidence of hepatic metastases was between 40% and 50%. These results, although strongly suggesting a treatment effect, imply that the dose of radiation, coupled with the 2-week break, was too low to deal with the regional burden of disease and the efficacy of 5-FU alone was inadequate to sterilize disease outside the treatment fields for most patients.
The European Organization for Research and Treatment of Cancer (EORTC) performed a multi-institutional, randomized trial in which 218 patients with periampullary cancers, including pancreatic adenocarcinoma, were randomized to receive surgery alone or surgery plus postoperative 5-FU–based chemoradiation.85 The radiation dose and fractionation were the same as in the GITSG trial (40 Gy in split-course fashion over 6 weeks). There were two differences in the delivery of 5-FU compared with the GITSG study. Concurrent 5-FU during RT was administered by continuous intravenous infusion, rather than bolus, during the first 3 days of each treatment sequence. Furthermore, no 5-FU was given after the concurrent chemoradiation. In the subset of 114 patients with pancreatic adenocarcinoma, patients in the chemoradiation arm (n = 60) had a median survival of 17.1 months versus 12.6 months in the pancreatectomy alone arm (n = 54). The 2-year OS for the two trial arms were 37% versus 23%, respectively, and 5-year OS was 20% versus 10% (p = .099). There were no differences in locoregional recurrence rates, which were high with both surgery alone (37 of 103, 36% of patients at risk) and postoperative chemoradiation (34 of 104, 33% of patients at risk). The EORTC concluded that there was no demonstrable benefit from postoperative chemoradiation for the total group of patients but that survival trends favored adjuvant postoperative chemoradiation for the 114 patients with pancreatic cancer.
However, several aspects of the EORTC trial design, analysis, and interpretation warrant comment. Patients with T3 lesions were excluded, and the pathologic basis for distinguishing between and including pancreatic and nonpancreatic periampullary lesions (which have different natural histories and prognoses than do pancreatic adenocarcinomas) was not made clear. Additionally, the adequacy of the retroperitoneal margin was not independently assessed, perhaps influencing the frequency of locoregional recurrence. Moreover, 20% of patients assigned to the chemoradiation trial arm never received that treatment (because of patient refusal, poor postoperative performance status, disease progression, etc.) but they were analyzed by intent-to-treat principles. Although this approach is statistically correct, one needs to consider that the chemoradiation group includes a sizable minority of patients who did not receive postoperative chemoradiation. Furthermore, unlike the GITSG trial, no chemotherapy was given after chemoradiation. Moreover, many have criticized the use of a two-sided log-rank test, and demonstrated that if a one-sided test had been used, the survival benefit of chemoradiation would have reached significance.86 Finally, the study lacked sufficient patient numbers to exclude a clinically significant 10% to 15% benefit from the addition of adjuvant chemoradiation to surgery. Thus some investigators consider the EORTC trial to be an underpowered study that provides additional circumstantial evidence to support a role for postoperative chemoradiation. However, the trial was updated in 2007 and continued to show no statistical survival advantage after a median follow-up of 11.7 years.87 Although this trial is used as evidence against chemoradiation, it has several methodologic flaws, as just listed.
An important trial for radiation oncologists to be aware of is the ESPAC-1 study,88 which had a complex design (three separate but concurrent phase III trials) and was initiated to evaluate the independent effects of adjuvant chemotherapy and chemoradiation in 541 patients with grossly resected pancreas cancer. This included a subset of 285 patients who underwent randomization with a 2 × 2 factorial design as follows: (1) observation; (2) concomitant chemoradiation alone (20 Gy in 10 fractions over 2 weeks with 500 mg/m2 5-FU IV bolus during the first 3 days of RT and then repeated after a planned 2-week break) followed by no additional chemotherapy; (3) chemotherapy alone (leucovorin 20 mg/m2 bolus followed by 5-FU 425 mg/m2 administered for 5 consecutive days repeated every 28 days for six cycles); and (4) chemoradiation followed by six cycles of adjuvant 5-FU/leucovorin. Investigators were also allowed to randomize patients into two separate but concurrent trials testing one of the main treatment comparisons (adjuvant chemotherapy vs. none: 188 patients; adjuvant concurrent chemoradiation vs. none: 68 patients). Background therapy was allowed before patients were entered into the latter two trials, and RT was performed according to the standard of the individual institutions in all three trials. In the initial analysis, a survival advantage for adjuvant chemotherapy was achieved only by merging data from the three separate randomized trials (median survival of 19.7 months in the 238 patients randomized to receive adjuvant chemotherapy vs. median survival rate of 14 months in the 235 patients randomized to no adjuvant chemotherapy, p = .005).89 The latest analysis of the ESPAC-1 trial analyzed only the patients randomized to the 2 × 2 factorial design (n = 289; no background therapy allowed). Patients randomized to receive adjuvant chemotherapy (two of the four arms, n = 147) had a survival advantage (2-year, 40% vs. 30%; 5-year, 21% vs. 8%; p = .009).88 Local recurrence was a component of relapse in 99 patients (34% of the 289 patients at risk, 63% of patients with relapse).
As noted in 2001 by Abrams and associates,90 major concerns regarding the design and execution of this trial include more than one randomization scheme (three separate but concurrent phase III trials), patients were allowed to receive “background” therapy in addition to protocol therapy in two of the three trials, patients did not have their disease restaged after resection and before adjuvant therapy, and there were no quality assurance guidelines for the delivery of radiation (i.e., no section in the protocol on appropriate field design, no central audit of radiation fields), which is contrary to the routine in North American cooperative group trials. ESPAC-1 was a trial of varying patient populations, and the nature of the differences in the patients cannot be known. Thus the validity of this analysis should be regarded with concern.
RTOG 97-04, a randomized phase III trial,91 evaluated whether gemcitabine before and after 5-FU–based chemoradiation would provide superior outcome to 5-FU before and after 5-FU–based chemoradiation. In this study, 518 patients with resected pancreatic cancer were treated with postoperative 5-FU–based chemoradiation (50.4 Gy in 28 fractions over 5.5 weeks plus concurrent protracted venous infusion of 5-FU). Patients were randomized to receive either 5-FU (250 mg/m2/day) given as continuous infusion over 3 to 4 weeks or gemcitabine (1000 mg/m2/wk) given for 3 of 4 weeks. Chemotherapy was given for a total of three cycles: one before chemoradiation and two cycles after chemoradiation. On subset analysis of patients with pancreatic head tumors, median survival and 3-year OS were 20.5 vs. 16.9 months and 31% versus 22% for the gemcitabine and 5-FU trial arms, respectively. These results neared statistical significance overall (p = .09) and reached significance on multivariate analysis (p

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


