Chapter 20 Neutron Radiotherapy
Fast Neutron Radiotherapy
Overview
The resulting energy transfer is in the range of 20 to 100 keV/µm compared with 0.2 to 2 keV/µm for the megavoltage photons and electrons used in conventional radiotherapy. It is this higher energy transfer that gives rise to the different radiobiologic properties of fast neutrons, which are advantageous in certain clinical situations. The higher relative biologic effectiveness (RBE) accounts for the different clinical response observed with neutrons as opposed to conventional photon irradiation. Fast neutrons have RBEs in the range of 3 to 3.5 in terms of most normal tissue late effects, RBEs in the range of 4 to 4.5 in terms of damage to the central nervous system, and RBEs in the range of 8 for salivary gland malignant tumors.1–3 High–linear energy transfer (LET) radiation causes a dense chain of ionizing events to both strands of the DNA and therefore makes DNA repair more difficult. Furthermore, high-LET radiation from fast neutrons is less sensitive to the reduced cell killing effects of hypoxia, with there being approximately equal cell killing under normoxic and hypoxic conditions.
Historical Perspective
Patients were first treated with fast neutron radiotherapy in 1938 by Robert Stone and co-workers4 at the Crocker Radiation Laboratory (later to become Lawrence Berkeley Laboratories). Two hundred forty patients were treated between 1938 and 1942. Many of these patients had received prior photon irradiation. There were significant radiation sequelae in the few long-term survivors such that clinical interest in fast neutron radiotherapy dropped off significantly for the next 20 years. Brennan and Phillips5 subsequently reviewed the initial work by Stone and colleagues and showed that an inappropriate value for the neutron RBE had been used in the dose calculations. Hence, many of those initial patients had been inadvertently overdosed. With a better understanding of the RBE of fast neutron radiotherapy in different tissue types, in the 1970s Catterall and coworkers6,7,8 resumed neutron clinical trials at Hammersmith Hospital in London, England. Their results indicated that many advanced head and neck cancers exhibited a good response with acceptable side effects. The interest in fast neutron radiotherapy grew so that at one point there were 39 different centers in North America, Europe, Asia, and Africa treating patients with fast neutrons. Clinical utility has been further elucidated through clinical trials and single-institution experience, and neutron radiotherapy now has fairly well defined and limited indications. There are currently only seven operating fast neutron radiotherapy centers throughout the world. These are listed in Table 20-1, along with some of their more important characteristics.
TABLE 20-1 Location of Operating Fast Neutron Radiotherapy Centers, 2009
| Location | Beam Reaction | Comments |
|---|---|---|
| United States | ||
| University of Washington Medical Center, Seattle, Washington | 50 MeV p→Be | Isocentric gantry and multileaf collimator |
| Fermi Laboratories, Batavia, Illinois | 66 MeV p→Be | Horizontal beam, fixed collimators with blocking inserts |
| Europe | ||
| Tomsk Polytechnical University, Tomsk, Russia | Cyclotron | Mean neutron energy 6.3 MeV |
| Technisch Universtät Munich, Munich, Germany | Fission neutrons | FRMII reactor, horizontal beam with multileaf collimator, mean neutron energy 1.9 MeV |
| Institute of Physics and Power Engineering, Obninsk, Russia | Fission neutrons | Horizontal beam |
| Asia | ||
| National Institute of Radiological Sciences, Chiba, Japan | 30 MeV d→Be | Vertical beam, multileaf collimator |
| Africa | ||
| National Accelerator Centre, Faure, South Africa | 66 MeV p→Be | Isocentric gantry and jaw collimator |
Be, beryllium, d, deuteron, FRMII, Forschungs-Nuetronenquelle Heinz Maier-Leibnitz; MeV, million electron volt; p, proton.
Salivary Gland Tumors
The therapeutic advantage of fast neutron radiotherapy over conventional radiotherapy is best established in salivary gland tumors. The RBE for salivary gland tumors is approximately 8, whereas for surrounding normal tissues, the RBE is 3 to 3.5.1 A typical neutron dose for a salivary gland cancer is approximately 18 to 20 nGy (neutron Gray). The approximate equivalent photon dose is 60 to 70 Gy equivalents (GyE) as far as normal tissues are concerned but it is in the range of 150 to 160 GyE as far as the tumor is concerned. The therapeutic gain factor for salivary gland tumors is therefore in the range of 2.3 to 2.6.
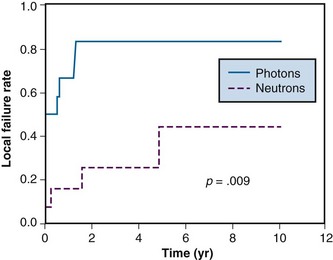
Early single-institution studies showed neutrons to be beneficial in the treatment of salivary gland tumors. These results led to a prospective randomized trial sponsored by the Radiation Therapy Oncology Group (RTOG) and the Medical Research Council (MRC) of Great Britain.9 Local control at 10 years was improved in the neutron arm (56% vs. 17%; p = .009). The final report showed a trend toward increased median survival of about 8 months in the neutron arm, but this was not statistically significant. However, the cause of death differed between the two subgroups. Metastatic disease was the main cause of death for the neutron patients, whereas local/regional tumor failure was the main cause of death for the photon patients. Of note, the study was stopped early for ethical reasons when 2-year survival data showed a strong trend in favor of the neutron patients. Local tumor control curves for this study are shown in Figure 20-1.
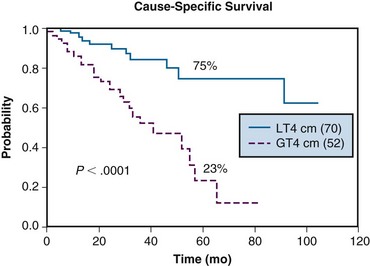
The University of Washington experience was reviewed by Douglas and colleagues.10,11 Two hundred seventy-nine patients treated with curative intent were included in the analysis. A majority (263 patients) had evidence of gross disease, with 141 having major salivary gland neoplasms and 138 having minor salivary gland neoplasms. The 6-year actuarial cause-specific survival rate was 67%. On multivariate analysis, stage I/II disease, minor salivary gland primary tumors, lack of base-of-skull involvement, and primary (rather than recurrent) disease were associated with improved survival rates. Improved locoregional control was associated with tumors having the following characteristics: greatest diameter less than 4 cm, no base-of-skull invasion, prior surgical resection, and/or no previous radiation therapy. The 6-year actuarial rate for freedom from the development of metastases was 64% for patients without lymph node involvement or base-of-skull involvement. There was a 6-year actuarial rate of 10% for developing RTOG grade 3 or 4 toxicity. Cause-specific survival curves for the major salivary gland patients as a function of tumor size are shown in Figure 20-2.
The poorer outcome of salivary tumors with base-of-skull involvement appears to be the result of the need to reduce the dose to portions of tumors that are adjacent to critical central nervous system structures (recall that the RBE for fast neutrons for central nervous system tissue is 4 to 4.5). With a standard 20-nGy dose to the involved site, the dose to the temporal tips could be approximately 80 photon GyE. Reducing the temporal lobe dose to a safe level sometimes necessitated blocking portions of tumor. In an attempt to compensate for the reduced neutron dose, a stereotactic radiosurgical boost with photon radiation has been instituted at the University of Washington. At 40 months there was improved local control compared with historically treated patients with skull base invasion who did not receive a stereotactic radiosurgical boost (82% vs. 39%; p = .04).12 Complications appear to be acceptable.
The use of both neutrons and photons in a composite “mixed beam” treatment has been explored by Huber and associates13 in a series of patients with advanced adenoid cystic carcinomas treated at the Heidelberg neutron facility. They found a 5-year local control rate of 75% for patients treated with neutrons alone compared with 32% for patients treated with “mixed beam” irradiation or with photons alone. It appears that patients who have a greater portion of their treatment with neutrons fare better. Distant metastatic disease once again prevented improved local control from translating into an increase in overall survival rates.
The neutron facility in Orleans has reported similar results for 59 patients treated with fast neutron radiotherapy.14 The 5-year local control rate was 69.5%, with a crude 5-year survival rate of 66% and a 5-year tumor-free survival rate of 64.5%.
Prostate Cancer
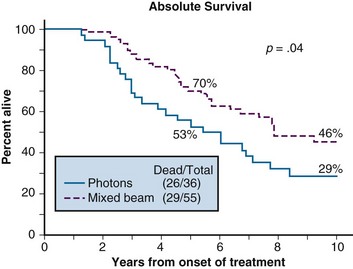
Prostate cancer is another tumor for which there has been significant clinical work using fast neutron radiotherapy. The National Cancer Institute (through RTOG 77-04) conducted a randomized trial for patients with T3, N0/N1 disease.15 One arm received a mixed beam (neutron/photon) dose to 70 GyE versus a second arm that received standard photons to 70 Gy. At the 10-year endpoint, survival rates (46% vs. 29%, p = .04) were improved in the mixed beam arm. There was also improved locoregional control (70% vs. 58%, p = .03) for the mixed beam subgroup. There was no difference in the rate of significant complications between the two arms. Survival curves for the patients in this study are shown in Figure 20-3.
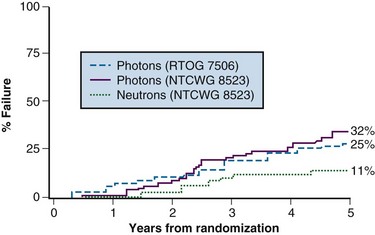
A follow-up randomized trial was conducted that compared 70-Gy standard photon irradiation with 20.4-nGy fast neutron therapy. This was carried out by the National Cancer Institute (NCI)–sponsored Neutron Therapy Collaborative Working Group (NTCWG) and included patients with high-grade T2 tumors or T3 to T4, N0 to N1, M0 tumors of any grade.16 With a median follow-up of 68 months, the 5-year actuarial locoregional failure rate was 11% for neutrons versus 32% for photons (p <.01). Actuarial overall survival and cause-specific survival rates were statistically equivalent. The incidence of severe complications was higher in the neutron group than in the photon group (11% vs. 3%). Complications were less severe and fewer in the centers that had more sophisticated beam-shaping abilities. Local failure curves for the patients in this study are shown in Figure 20-4.
Following the randomized trials, additional studies were conducted at several centers in the United States,17,18,19,20,21 Europe,22,23 and Asia.24,25 These single-institution results showed good local and regional control and appeared to corroborate the results of the randomized trials described earlier.
Sarcomas
Sarcomas are generally considered to be among the more “radioresistant” histologic types of tumors and so would fall into the category of tumors thought to be more responsive to high-LET radiation.1 A retrospective review by Schwarz and colleagues26 reports on 1171 soft tissue sarcoma patients from 11 European centers treated with fast neutron radiotherapy. In those patients with either inoperable tumors or gross disease after surgery, the local control rate was approximately 50%. Toxicity was higher than what was generally seen with photon irradiation. The local control rates were thought by the authors to be better than what would have been expected with standard radiotherapy. This conclusion is supported by other single-institution studies.27
Other Tumor Types
Fast neutron radiation has been tested on a variety of other tumor types. Generally, the rationale for the use of fast neutrons came from trying to overcome a perceived limitation of standard photon irradiation. A good example of this is malignant glioma of the brain. Dose-escalation studies with photons have failed to increase overall survival rates.28 By definition, glioblastoma multiforme tumors have associated areas of necrosis that are often surrounded by regions of hypoxia, which might make the tumors more radioresistant. Studies of malignant gliomas in the 1970s and 1980s used neutrons either alone or in combination with photons.29 None of these initial trials showed an improvement in overall survival rates with the addition of neutrons. However, with relatively high doses of fast neutrons alone, autopsy and second-look surgical data indicated that tumor cells were sterilized in the treated region.30 Unfortunately, there was also significant coagulative necrosis caused by the neutron irradiation, which indicated too much damage to normal brain tissue. A more recent study used fluorodeoxyglucose–positron emission tomography (FDG-PET) scanning to determine the final boost volume that received 18 nGy.31 Only 10 patients were treated and all exhibited tumor progression by 39 weeks, perhaps because of the restricted fields that were employed. Gliosis and microvascular sclerosis consistent with radiation injury were noted in regions of the contralateral brain receiving 6 to 10 nGy. Much of the current interest in neutron radiotherapy for malignant gliomas is focused on BNCT, which is discussed later in this chapter.
Boron Neutron Capture Therapy
Historical Perspective
The basic idea for BNCT dates to 1936, when Locher32 proposed treating malignant tumors with low-energy thermal neutrons via a capture process with 10B. A few years later, Kruger33 and Zahl and colleagues34 experimentally verified some of the basic tenets of this concept and demonstrated the high RBE of the resulting helium-4 (4He) and lithium-7 (7Li) fission fragments. The theoretical advantage of “tagging” the tumor-specific carrier with an innocuous substance such as 10

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


