Notochordal Tumors
Hannah D. Morgan
In human embryos, the notochord is a rod of cells on the ventral aspect of the neural tube. It is the foundation of the spinal column, as the vertebral segments are formed around it. In the adult, notochord remnants form the nucleus pulposus of vertebral disks. Chordomas are slow-growing malignant tumors of bone arising from the remains of notochordal tissue almost exclusively in the axial skeleton and exhibiting notochordal differentiation. There is frequently an associated soft tissue mass, which most commonly extends anteriorly but may have intraspinal extension as well. Chordomas are typically only locally aggressive, but occasionally they do metastasize. Prompt diagnosis of the tumor followed by complete surgical resection with or without adjuvant radiation therapy offers the best clinical outcome.
Pathogenesis
Etiology
Chordomas are low-grade malignant neoplasms of bone arising from vestigial notochordal remnants that are almost exclusively found in the midline of the sacrococcygeal, spheno-occipital (cranial), and mobile spine regions.
Epidemiology
3% to 4% of primary bone tumors
Incidence rate in United States: 0.08 per 100,000
Male > female (male:female incidence rate 0.1–0.06 per 100,000)
Median age: 58 years; rare <40 years; extremely rare in first decade
Race: 91% Caucasian, 2% African-American, 7% other
Anatomic distribution: 30% to 50% sacral, 30% cranial, 15% to 30% spinal
Younger patients and females have propensity for cranial tumors.
Older patients more likely to have sacral site
Pathophysiology
Chordomas are soft, grayish, lobular masses. They may have gelatinous portions. They may cause expansion of the cortical bone, and many have associated soft tissue masses. Histologically, the tumors are composed of cords or nests of cells with vacuolated cytoplasm. Mitoses are infrequent. The hallmark cells are physaliferous cells (cells with bubbly cytoplasm surrounding the nucleus), although they may be sparse or absent altogether. Occasionally there is chondroid differentiation (Fig. 6.5-1).
Classification
Grade and stage: most chordomas are low grade and localized
Rarely patients present with metastatic disease.
Variants: dedifferentiated and chondroid (skull base) described
Diagnosis
Physical Examination and History
Clinical Features
Pain and neurologic deficits are usual symptoms.
Sacral: bowel, bladder, and sexual dysfunction
Clival: cranial nerve dysfunction (facial weakness, double vision)
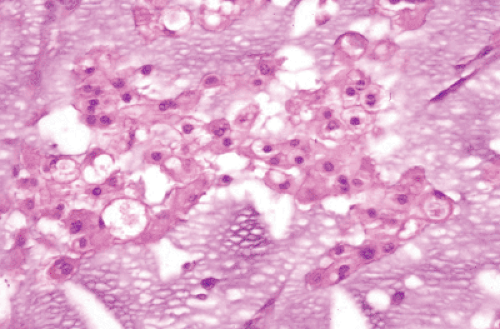
Figure 6.5-1 Chordoma.
Mobile spine: back pain, leg pain, autonomic dysfunction
Delay in diagnosis of months to years common, due to chordoma’s slow growth and deep locations
Physical examination: thorough neurologic examination and rectal examination (for sacrococcygeal chordomas)
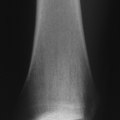
Radiologic Features
Plain radiographsRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree