Ewing Sarcoma and Primitive Neuroectodermal Tumor of Bone
Bruce Rougraff
Ewing sarcoma was a feared cancer of childhood, with very few survivors, prior to the use of chemotherapy, surgical resection, and radiation. The disease manifests as chronic increasing pain in the area of a lytic, destructive bone lesion of flat bones and the diaphysis of long bones. The initial presentation is frequently confused with osteomyelitis, and it can be mistakenly treated as that for a period of time before the diagnosis is established. Ewing sarcoma and a less virulent related disease, primitive neuroectodermal tumor of bone (PNET), metastasize to lung,
bone, and bone marrow most frequently. Current management includes biopsy, staging, neoadjuvant chemotherapy, surgical resection and/or radiation, and further chemotherapy. The 5-year survival rate is 60% to 65% for nonmetastatic disease and 25% to 30% for metastatic disease.
bone, and bone marrow most frequently. Current management includes biopsy, staging, neoadjuvant chemotherapy, surgical resection and/or radiation, and further chemotherapy. The 5-year survival rate is 60% to 65% for nonmetastatic disease and 25% to 30% for metastatic disease.
Pathogenesis
Etiology
Unknown; associated with reciprocal translocation of chromosomes 11 and 22 (90% of cases), which involves bands q24 and q12 of both chromosomes respectively
This results in a new chimeric EWS/FLI-1 fusion product, which produces the EWS/FLI-1 or MIC2 protein, stained for by the CD99 immunohistochemistry marker.
Epidemiology
Third most common primary bone sarcoma (after osteosarcoma and chondrosarcoma, respectively)
Three times less common than osteosarcoma
Rare in African-Americans (0.5% of Ewing cases); peak incidence in the second decade of life
Male:female ratio 1.3:1
Pathophysiology
Sheets of monotonous, small, round blue cells with indistinct cytoplasm (Fig. 6.2-1)
Glycogen granules in the cytoplasm can be seen after periodic acid Schiff (PAS) staining or with electron microscopy.
PAS-positive granules sensitive to digestion with diastase
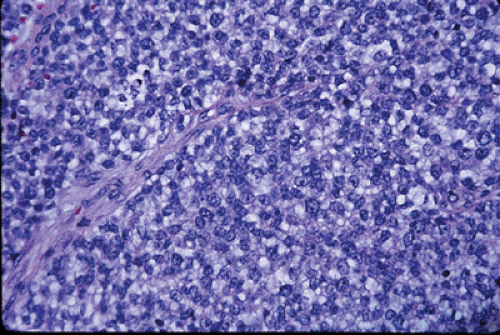
Figure 6.2-1 This hematoxylin-and-eosin (H&E) staining shows typical Ewing sarcoma features of monotonous sheets of small, round blue cells with indistinct cytoplasm.

Figure 6.2-2 This CD-99 immunohistochemical staining shows positivity that is consistent with Ewing sarcoma. Cytogenetics is used to confirm Ewing/PNET (t11:22).
The nuclear chromatin is finely granular, with one to three small nucleoli per nuclei.
CD99 immunohistochemistry marker stains for EWS/FLI1 fusion or MIC2 protein, which is present in 90% of cases. (Fig. 6.2-2)
Classification
Ewing sarcoma: most common, least differentiated, worst prognosis
PNET: more neural differentiation, better prognosis
Askin’s tumor: primary in thoracopulmonary region, best prognosis
Diagnosis
Clinical Features
Typical age at diagnosis: 5 to 30 years
Rare in patients <5 years old; this distinguishes it from metastatic neuroblastoma
Usually presents as a painful mass
May be accompanied by fever and weight loss, which are poor prognostic signs
Radiographic Features
LocationRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



