NORMAL VARIANTS
EMPTY SELLA
The sella may not be completely filled with tissue. When the sella is partially filled with CSF in the suprasellar cistern, it is referred to as an empty sella (Fig. 20-4). A partially empty sella is a common incidental finding and usually should be considered a normal variation in anatomy. The empty sella may be related to incomplete formation of the diaphragma sella, allowing CSF into the pituitary fossa (see Chap. 11). A partially empty sella can be seen in association with pseudotumor cerebri, hydrocephalus, previous pituitary surgery, or a previous pituitary mass that has shrunk. It can also be seen after irradiation, after trauma, or as sequela of apoplexy. Occasionally, an empty sella is associated with a CSF leak or fistula. The term empty sella syndrome has been used to describe a variable clinical constellation of findings, such as headache, endocrine dysfunction, and visual disturbances, which are seen in association with a partially empty sella.15
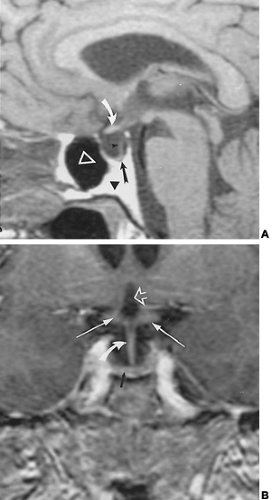 FIGURE 20-4. Empty sella. A, Sagittal T1-weighted non–contrast-enhanced image. Note that the pituitary stalk (small black arrowhead) extends all of the way to the floor of the sella (thick black arrow). The pituitary gland is very thin and not well marginated. In this case, the clivus (large black arrowhead) has a large amount of fat generating a high signal intensity region. The other normal structures include the optic chiasm (curved white arrow) and sphenoid sinus (open white arrowhead). B, Coronal contrast-enhanced T1-weighted image. The pituitary stalk (curved white arrow) is seen extending all of the way to the floor of the sella. The gland is seen as a thin, “crescent-shaped” structure (thick black arrow) at the base of the sella. Other labeled structures include the hypothalamus and optic chiasm (white straight arrows) and the anterior third ventricle (open white arrow). |
With an empty sella, the sellar bony margins may be expanded, forming an oval or J shape on plain radiograph or
CT. It is often of normal size. The CSF spaces extend into the sella; the pituitary gland may be normal, small, or large in size. The optic nerve, optic chiasm, and optic tracts may herniate into the empty sella. The main finding is visualization of the pituitary stalk extending into the fossa, which is the best way to distinguish an empty sella from a cystic mass.
CT. It is often of normal size. The CSF spaces extend into the sella; the pituitary gland may be normal, small, or large in size. The optic nerve, optic chiasm, and optic tracts may herniate into the empty sella. The main finding is visualization of the pituitary stalk extending into the fossa, which is the best way to distinguish an empty sella from a cystic mass.
CONGENITAL ANOMALIES
HYPOPLASTIC PITUITARY
The pituitary gland can be congenitally hypoplastic. Many of these patients present with a combination of endocrine deficiencies in childhood. Plain radiographs of the sella demonstrate a small sella turcica, which may measure only a few millimeters in dimension. The presence of a small bony cavity is a sign that the pituitary gland never developed to a normal size rather than an indication of some type of destructive process. Although CT and MRI confirm that the pituitary gland is small, the hypothalamus and other adjacent structures usually appear intact.
ECTOPIC POSTERIOR PITUITARY GLAND
An ectopic posterior pituitary gland is a relatively common etiology for hypopituitarism and growth hormone (GH) disturbances in young patients.16 On plain radiograph and CT, the pituitary fossa may be small or normal in size, with an ectopically placed pituitary gland. The pituitary gland itself may be hypoplastic or normal in appearance. Because CT and plain radiographs cannot differentiate the anterior and posterior lobes of the pituitary gland or demonstrate the nodule adjacent to the hypothalamus, there is really no role for these procedures in the evaluation of an ectopic posterior pituitary.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


