Myogenic, Lipogenic, and Epithelial Bone Sarcomas
Hannah D. Morgan
Leiomyosarcoma and liposarcoma of bone and adamantinoma are all rare osseous malignancies, each constituting less than 1% all bone sarcomas. Patients with leiomyosarcoma and liposarcoma of bone should be carefully examined to ensure that the bony lesion is a primary tumor and not a metastasis from a soft tissue malignancy. Adamantinoma should be always be considered in the differential diagnosis of a tibial aggressive lesion.
Pathogenesis
Etiology
Leiomyosarcoma: arises from smooth muscle cells of intraosseous blood vessels
Liposarcoma: etiology unknown; immature adipose tissue
Adamantinoma: presumed ectopic epithelial cell residues
Epidemiology
Leiomyosarcoma
Extremely rare; <0.1% of all bone sarcomas
Male = female
First through ninth decades; mean age 45 to 50 years
Femur/tibia > humerus > ilium in extragnathic sites
Liposarcoma
One of the rarest primary bone tumors
Second through sixth decades; typically third and fourth decades
Major long tubular bones affected
Adamantinoma
∼0.4% of bone sarcomas
Male:female 3:2
Young adults and children (mean age 30 years); typically older than osteofibrous dysplasia
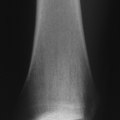
85% involve tibia (especially anterior aspect); 10% tibia and fibula
Pathophysiology
Leiomyosarcoma
Spindle-shaped cells with eosinophilic cytoplasm and cigar-shaped nuclei arranged in bundles intersecting at right angles (Fig. 6.7-1)
Immunohistochemistry: positive vimentin (as for all sarcomas), positive smooth muscle actin
Liposarcoma
Either pleomorphic or round cell–rich high-grade lesion
Signet-ring lipoblasts may be seen.
Adamantinoma
Epithelial cells surrounded by spindle-shaped fibrous tissue; little pleomorphism (Fig. 6.7-2)
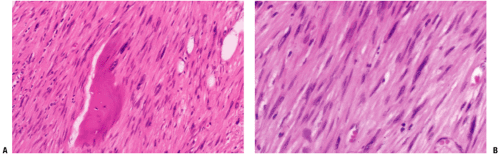 Figure 6.7-1 Leiomyosarcoma of bone. Note pleomorphic elongated cells with cigar-shaped nuclei. |
Classification
Leiomyosarcoma: 80% of tumors are high-grade malignancies of smooth muscle origin
Liposarcoma: high-grade lesions of immature adipose tissueRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree