Benign mesenchymal neoplasms may arise within the urinary tract, although it is notable that they are less common than their malignant counterparts. Primary sarcomas of the urinary bladder are rare, more common in males than in females, and comprise less than 0.5% of malignant tumors arising at this site (1, 2, 3, 4). The majority are of muscle origin, and while myosarcomas may occur in any age group, rhabdomyosarcomas (RMS) predominate in children, while leiomyosarcomas (LMS) predominate in adults.
LEIOMYOMA
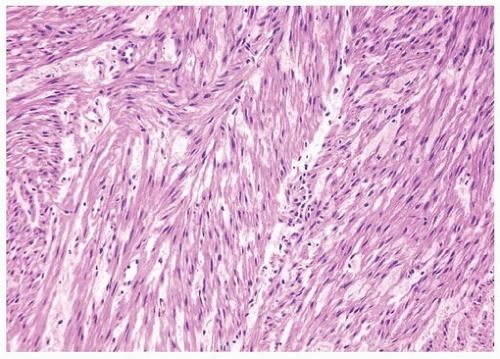
Leiomyoma is the most common benign mesenchymal neoplasm of the urinary bladder, exhibiting the same morphologic features seen at other sites (5, 6, 7) (Figs. 11.1, 11.2) (efig 11.1). On transurethral resection (TUR), there is a tendency to overlook the neoplastic smooth muscle as fragments of muscularis propria, as the presence of circumscribed nodules cannot typically be appreciated. However, in contrast to the well-formed bundles of muscularis propria, leiomyomas in the context of a clinical/cystoscopic mass lesion are composed of large compact sheets of intersecting smooth muscle fascicles (Fig. 11.3). Typically, they exhibit low cellularity and minimal or no cytological atypia or mitoses. We have anecdotally seen leiomyomas of the bladder with degenerative atypia (symplastic leiomyoma), although there is no reported information on their clinical or biologic potential (see “Leiomyosarcoma” section). Leiomyomas express smooth muscle actin and desmin.
LEIOMYOSARCOMA
LMS are the most common sarcoma encountered in the urinary bladder in adults, although there have been cases reported in children (1, 3, 5, 8). Although most present de novo, isolated cases have been reported subsequent to chemotherapy with cyclophosphamide (9, 10, 11, 12). The tumors are usually well circumscribed, may protrude into the lumen, and ulcerate the overlying urothelium. Size is variable, although some may measure up to 20 cm. They occur more frequently in males than in females in a ratio of 2:1. Morphologic features are identical to those seen in other sites, including the presence of interlacing fascicles of spindle cells with variable amounts of eosinophilic cytoplasm with mild to marked nuclear atypia (Fig. 11.4) (efigs 11.2-11.7). Some tumors may have prominent myxoid change, and others may have a prominent epithelioid morphology. The majority of cases will demonstrate tumor necrosis and mitotic activity of 10 per 10 high-power fields or more. Although most smooth muscle tumors of the bladder are overtly either benign or malignant, there are some tumors with low cellularity yet with atypia or rare mitotic activity. In the uterus, these lesions would be classified as benign, even if accompanied by a few readily identifiable mitotic figures. As there are no follow-up data in the literature for comparable lesions in the bladder, it may be more prudent to designate these lesions as “atypical smooth muscle tumors” describing their findings and stating that their biological behavior is unknown. For those lesions without mitotic figures, it can be added that it is likely that they will behave in an indolent fashion.
FIGURE 11.1 Leiomyoma.
FIGURE 11.2 Leiomyoma (higher magnification of Fig. 11.1).
FIGURE 11.3 Leiomyoma composed of irregular sheets of smooth muscle (left) as opposed to well-formed discrete smooth muscle bundles of normal muscular propria (right).
Sarcomatoid carcinoma may mimic LMS and must be excluded by adequate sampling of the specimen (to identify a carcinomatous or in situ component) and appropriate histochemical and immunohistochemical studies. LMS of the bladder are so rare that this diagnosis should be made only after excluding all other possibilities, particularly sarcomatoid carcinoma but also secondary involvement from an adjacent organ. LMS (approximately 50%) may express some to occasionally a moderate degree of cytokeratin (13, 14) but typically are composed of regular intersecting fascicles as opposed to the more haphazard growth pattern of sarcomatoid carcinoma and typically relatively diffusely express smooth muscle actin and muscle specific actin. One must also rule out reactive spindle cell lesions, which may occur after local surgery or trauma. These reactive lesions are composed of spindle cells that may also consistently express smooth muscle markers by immunohistochemistry but are of myofibroblastic origin (see below). Over two thirds of LMS will demonstrate immunoreactivity of both smooth muscle actin (1A4) and muscle-specific actin (HHF-35). Desmin will be positive in some of the cases, whereas epithelial membrane antigen is usually negative. It has been suggested that caldesmon will be positive in LMS but negative in myofibroblastic lesions (15) (Table 11.1). A recent review of the Surveillance, Epidemiology, and End Results (SEER) database found that grade, advanced disease at diagnosis, and failure to undergo surgical excision correlated with poor outcome (16).
FIGURE 11.4 Leiomyosarcoma.
TABLE 11.1 Spindle Cell Neoplasms of the Bladder: Immunoreactivity
a Sarcomatoid carcinomas with mesenchymal differentiation may express muscle markers.
RMS, rhabdomyosarcoma; LMS, leiomyosarcoma; SFT, solitary fibrous tumor; IMT, inflammatory myofibroblastic tumor; PMP, pseudosarcomatous myofibroblastic proliferation; SC, sarcomatoid carcinoma; Vim, vimentin; SMA, smooth muscle actin (clone 1A4); MCA, muscle common actin (clone HHF-35); EMA, epithelial membrane antigen (clone MC5); ALK, anaplastic lymphoma kinase; +, positive in >75% of cases; +/−, positive in >50% of cases; −/+, positive in <50% of cases; −, negative in <5% of cases.
RHABDOMYOSARCOMA
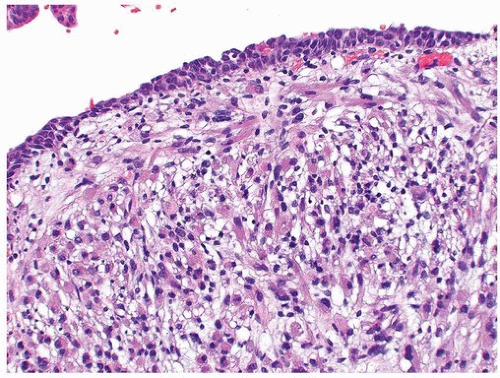
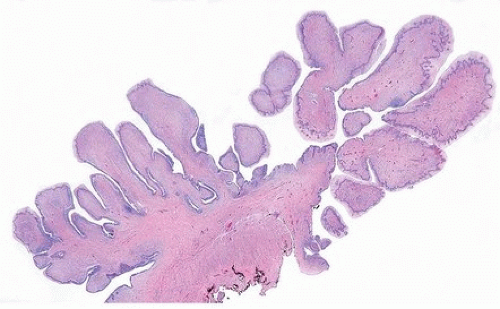
In children, 20% to 27% of RMS arise in the genitourinary tract. The bladder, prostate, and paratesticular region are the most common primary sites in males and the bladder and vagina in females (14, 17, 18, 19, 20) (Figs. 11.5, 11.6) (efigs 11.8, 11.9). The mean age at diagnosis for vesical RMS is 4 years. Most are embryonal rhabdomyosarcoma and exophytic (polypoid), with or without a “botryoid” component. Microscopically, the botryoid variant of RMS has a superficial condensation of tumor cells (so-called cambium layer), including strap cells and rhabdomyoblasts, located immediately beneath the urothelium (Figs. 11.7, 11.8). The underlying stroma is hypocellular and myxoid, and here, the tumor cells may have a more bland appearance. In other polypoid tumors, the neoplastic cells are diffusely distributed throughout. A significant percentage of vesical RMS does not have an exophytic component, and in these, the tumor cells infiltrate the bladder wall diffusely (20). The spindle cell and alveolar variants of RMS may be rarely encountered. Typical rhabdomyoblasts and cross striations are seen frequently in exophytic RMS but rarely seen in the spindle cell and alveolar types. Rare cases of vesical rhabdomyosarcoma have been described in adults, and these may have embryonal, pleomorphic, or alveolar patterns (19). Rhabdomyosarcoma should enter in the differential diagnosis of all spindle and myxoid lesions of the genitourinary tract in the pediatric age group. Tumor cells will be at least focally immunoreactive for desmin and myogenin, or myoD1, the latter two markers in a nuclear distribution (14). Immunoreactivity for myoglobin is also diagnostic, although it is positive in a minority of cases (Table 11.1).
FIGURE 11.5 Rhabdomyosarcoma.
FIGURE 11.6 Rhabdomyosarcoma.
FIGURE 11.7 Botryoid variant of rhabdomyosarcoma.
FIGURE 11.8 Cambium layer of botryoid variant of rhabdomyosarcoma (higher magnification of Fig. 11.7).
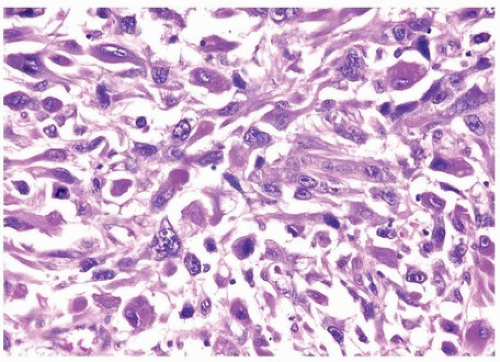
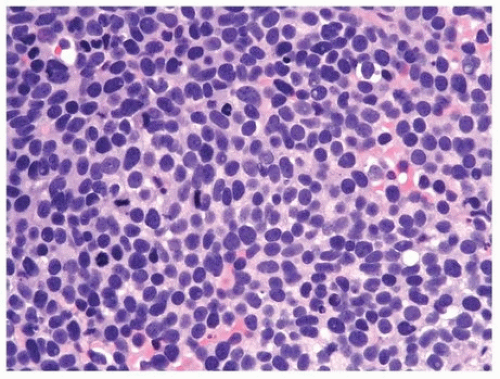
A subset of these tumors may have remarkable overlap in morphology with small cell carcinoma, as the typical alveolar morphology may not be obvious and there may be greater degree of anaplasia (Fig. 11.9). Synaptophysin immunoreactivity, which can be seen in these tumors, further complicates this differential diagnosis, although myoD1, myogenin, and desmin should help confirm the diagnosis (21).
Presently, there is no specific translocation associated with embryonal rhabdomyosarcoma, although they exhibit a significant amount of genomic instability in the form of copy number abnormalities. Fusion of FOXO1 on chromosome 13 with either PAX3 on chromosome 2 or PAX7 on chromosome 1 is present in up to 75% of alveolar RMS and preferentially in advanced or clinically aggressive tumors. The rare spindle cell or sclerosing variants, more commonly seen in adults, exhibit somatic mutations of MYOD1 and/or PIK3CA.
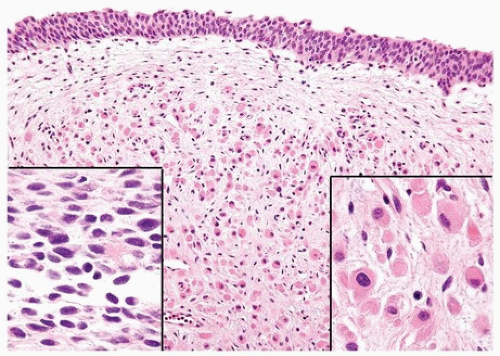
In general, RMS have a poor prognosis in adults. Combination therapy with surgery and chemotherapy has greatly improved survival in the pediatric age group. Studies have suggested that exophytic RMS have a better prognosis than those that infiltrate the bladder wall diffusely (20). Patterns of embryonal RMS with a better prognosis include the spindle cell, botryoid, and tumors lacking diffuse anaplasia (criteria similar to Wilms tumors). Alveolar and pleomorphic variants are associated with a relatively poor outcome. Interestingly, treated tumors commonly exhibit morphologic evidence of “maturation” as evidenced by a greater number of myoblasts and cross striations (Fig. 11.10).
FIGURE 11.9 Rhabdomyosarcoma resembling small cell carcinoma.
FIGURE 11.10 Rhabdomyosarcoma postchemotherapy. Areas of the tumor showed mature rhabdomyoblasts (right inset), while others demonstrated cellular, more poorly differentiated sarcoma (left inset).
MYOFIBROBLASTIC PROLIFERATIONS OF THE BLADDER: INFLAMMATORY MYOFIBROBLASTIC TUMOR AND REACTIVE PSEUDOSARCOMATOUS MYOFIBROBLASTIC PROLIFERATION
Lesions of myofibroblastic origin that involve the urinary bladder mimic sarcoma or sarcomatoid carcinoma. They have been described under a variety of names including inflammatory pseudotumor, pseudosarcomatous myofibroblastic tumor, pseudosarcomatous myofibroblastic proliferation (PMP), pseudosarcomatous fibromyxoid tumor, nodular fasciitis, postoperative spindle cell nodule, and most recently inflammatory myofibroblastic tumor (IMT). It is evident that myofibroblasts can give rise to two types of lesions, one reactive (PMP) and the other neoplastic (IMT). Importantly, both have significant overlapping histologic features (efigs 11.10-11.49). In 1984, Proppe et al. (22) reported on nine cases of spindle cell tumors, two of which involved the bladder and three the prostatic urethra, all appearing within months of a TUR. They named the lesions “postoperative spindle cell nodules of the genitourinary tract.” These apparently benign proliferative lesions are characterized histologically by plump, stellate, or elongated spindle cells, which infiltrate the bladder wall and focally can destroy muscle. The lesion can be quite cellular. A prominent feature of these tumors is a delicate network of small blood vessels in an edematous or myxoid stroma with little to moderate collagen deposition. Mitotic figures may be present and even frequent, but they are not atypical. The surface urothelium is usually ulcerated with an acute inflammatory cell infiltrate superficially and chronic inflammatory infiltrate scattered throughout the remainder of the lesion.
Only gold members can continue reading. Log In or Register to continue