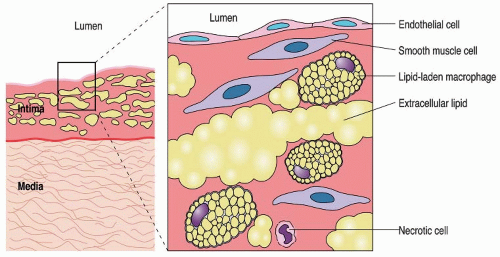
 FIGURE 94.1 Fatty streak of atherosclerosis. The fatty streak, composed largely of foamy macrophages, is presumed to be an early stage in the formation of atherosclerotic lesions. Note the intimal thickening in the left panel and the infiltrating cells in the enlargement on the right. (From Rubin R, Strayer DS. Rubin’s pathology: clinicopathologic foundations of medicine, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008.) |
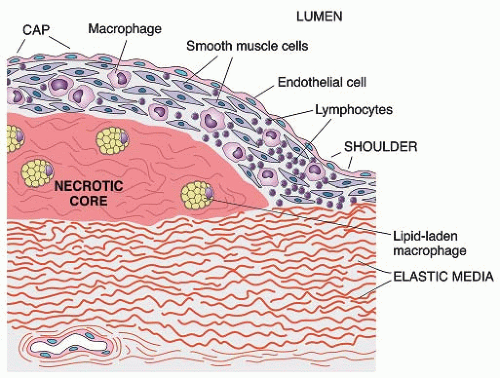 FIGURE 94.2 Fibrofatty plaque of atherosclerosis. In this fully developed fibrous plaque, the core contains lipid-filled macrophages and necrotic SMC debris. The “fibrous” cap is composed largely of SMCs, which produce collagen, small amounts of elastin, and glycosaminoglycans. Also shown are infiltrating macrophages and lymphocytes. (From Rubin R, Strayer DS. Rubin’s pathology: clinicopathologic foundations of medicine, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008.) |
addition, smoking directly influences atherosclerosis by causing endothelial dysfunction, inflammation, and coagulation within the vascular bed.21 Individuals who smoke are at risk for cardiovascular events, such as sudden cardiac death, nonfatal myocardial infarction, and ischemic stroke. Active smokers are at a 4.6-fold increased risk of developing PAD compared to nonsmokers,14 and smoking is associated with a threefold increased risk of CLI, with both PAD severity and progression directly correlated to the number of cigarettes consumed.
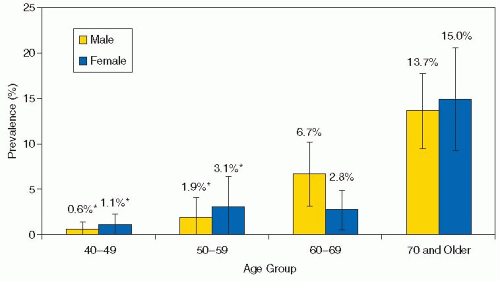 FIGURE 94.3 Prevalance of PAD in adults over 40 years by age and gender. (Reprinted from Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation 2004;110:738-743, with Permission.) |
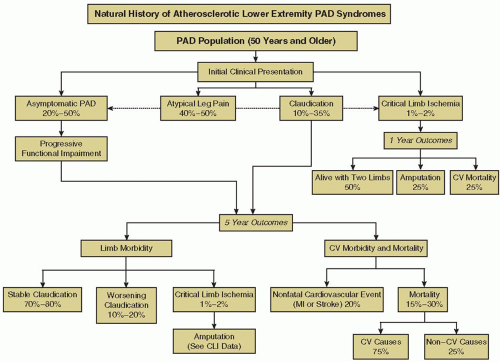 FIGURE 94.4 Natural history of lower extremity PAD. Individuals may be asymptomatic or present with symptoms of leg pain or CLI. All individuals with PAD face a risk of progressive limb ischemia symptoms, increased cardiovascular ischemic event rate, and increased mortality. CV, cardiovascular; MI, myocardial infarction. (Reprintedfrom Hirsch AT, Haskal JZ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation 2006;113:e462-e654, with permission. ©2006 American Heart Association, Inc.) |
and Rutherford classification systems may be used to organize PAD severity systematically based on the degree of leg ischemia (Table 94.1). Individuals who present with symptoms suggestive of intermittent claudication or CLI should undergo objective testing to confirm the presence of PAD. Acute limb ischemia (ALI) occurs due to a sudden interruption of the blood flow to an extremity, with patients presenting with a combination of limb pain, pallor, pulselessness, paresthesia, or paralysis signifying threatened limb viability.16
 FIGURE 94.5 Ischemic ulcers and gangrene in a patient with CLI. (From Topol EJ, Califf RM, et al. Textbook of cardiovascular medicine, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006.) |
Table 94.1 Classification of PAD: Fontaine stages and Rutherford categories | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
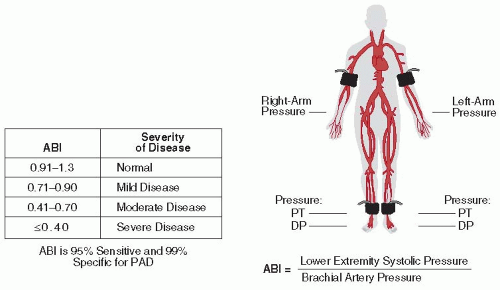 FIGURE 94.6 Measurement of the ABI. DP, dorsal pedis artery; PAD, peripheral arterial disease; PT, posterior tibial artery. (Adapted from Topol EJ, Califf RM, et al. Textbook of cardiovascular medicine, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006.) |
present.42 Due to the accuracy of the ABI in predicting PAD, and the increased cardiovascular risk associated with an abnormal ABI measurement, patients who are asymptomatic with an ABI ≤0.9 should undergo lifestyle and pharmacologic risk factor modification in accordance with a diagnosis of vascular disease.
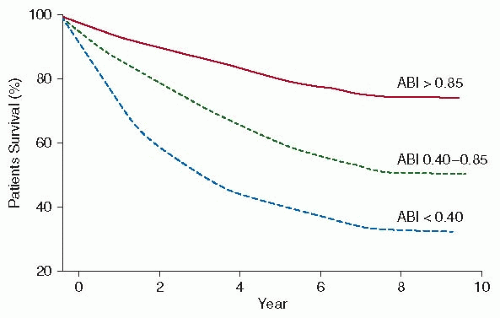 FIGURE 94.7 Survival with PAD severity based on the ABI. (From Topol EJ, Califf RM, et al. Textbook of cardiovascular medicine, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006.) |
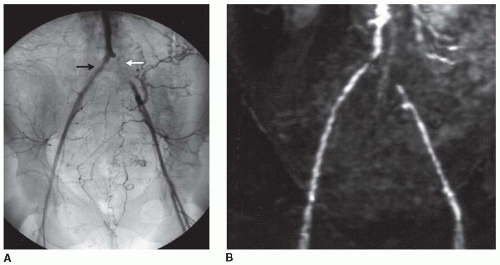 FIGURE 94.8 A: Pelvic arteriogram of a 75-year-old female with bilateral hip claudication. The study demonstrates diffuse infrarenal aortic atherosclerosis, right common iliac artery stenosis (black arrow), and left common iliac artery occlusion (white arrow) with external iliac artery reconstitution via collaterals. B: Corresponding MRA with 2-D gadolinium-enhanced technique. (From Baim DS. Grossman’s cardiac catheterization, angiography, and intervention, 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006.) |
an alternative antiplatelet agent to aspirin for cardiovascular risk reduction in patients with PAD. The development of severe neutropenia, a potentially fatal side effect, has been reported in 2.1% of patients prescribed ticlopidine, which has significantly limited its use in clinical practice.60
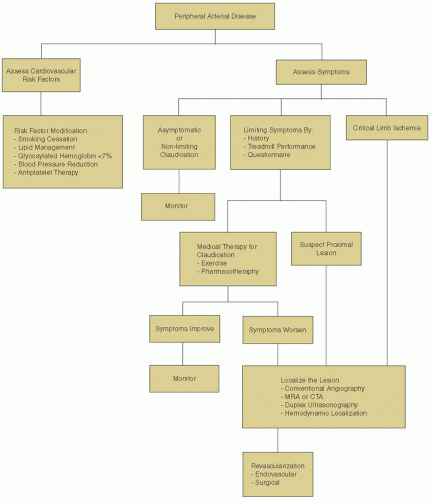 FIGURE 94.9 Overview of the management of patients with asymptomatic PAD, intermittent claudication, or CLI. (Adapted from Hiatt WR. Medical treatment of PAD and claudication. N Engl J Med 2001;344(21):1608-1621, with permission. © 2001, Massachusetts Medical Society. All rights reserved.) |
Table 94.2 Treatment guidelines for cardiovascular risk reduction in patients with PAD | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
Related posts:
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


