Mantle cell lymphoma is a relatively rare subtype of lymphoma with a great deal of heterogeneity, both clinically and biologically. Since its recognition as a separate entity in the early 1990s though, consistent efforts have led to a significant improvement of overall survival, from a median overall survival of 2.5 years initially to 5-7 years currently. This decades-long and stepwise progress, summarized in the article, definitely accelerated recently, shedding light on a changing paradigm.
Key points
- •
Mantle cell lymphoma (MCL) outcome has improved thanks to the achievement of deeper remission (complete remission [CR] and molecular CR), which translates into much longer progression-free survival (>5 years) and greater overall survival (OS).
- •
Maintenance rituximab in responders (post-R-CHOP [rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone] and post-high-dose therapies–autologous stem cell transplantation) improves duration of response and might improve OS in some cases.
- •
Novel therapies (bortezomib, lenalidomide, ibrutinib) which have shown durable responses in the relapsed/refractory setting, including in chemorefractory patients, offer an opportunity to build up on current regimens as either combination and/or maintenance strategies, while also offering hope for non-chemotherapy-based options, particularly in elderly MCL patients.
- •
Integrating biologicals into current regimens will likely improve quality and durability of response in both combination and maintenance settings.
- •
Biologicals-only combinations might help develop non-chemotherapy-based options, particularly in elderly MCL patients.
- •
A shift in the MCL paradigm is definitely seen. Finally, a greater awareness of biological heterogeneity might serve to stratify patients better in the clinic.
Background
The field of mantle cell lymphoma (MCL) has changed dramatically since its recognition as a separate entity more than 30 years ago. The concept of mantle-zone lymphoma first introduced in 1982 by Weisenburger and colleagues was confirmed by the International Lymphoma Study Group in 1992 and refined in the Revised European-American Lymphoma and World Health Organization classification in 1994. MCL recognition was based on its distinct morphologic and molecular features (hallmark t(11;14) translocation), but also its immunophenotype and distinct clinical course, with much poorer outcome among “indolent lymphomas.”
MCL represents 6% to 10% of non-Hodgkin lymphomas with a median age at diagnosis in the mid to late 60s and a clear predominance in men (ratio 3:1). Some data suggest a possible increase in MCL incidence over the last two decades, albeit likely reflecting improved diagnostics. Although most MCL cases are thought to derive from an antigen-naive pre-germinal center B cell, there is definite evidence of cases with restricted immunoglobulin gene repertoire (particularly IGHV3-21 and IGHV4-34 genes), which together with precise somatic hypermutation patterns suggest a role for chronic antigenic stimulation. Moderate associations with MCL risk have been reported for Borrelia burgdorferi infection, lifestyle-related factors, family history of hematopoietic malignancies, or genetic susceptibility (interleukin-10 and tumor necrosis factor genes), while others suggest molecularly defined antigenic specificity for B-cell receptor (BCR) in some series.
The t(11;14)(q13;q32) translocation that juxtaposes the proto-oncogene CCND1 at 11q13 to the immunoglobulin heavy chain complex ( IGH ) at chromosome 14q32 is considered the primary oncogenic mechanism (although not sufficient) for the development of MCL. This translocation forces the constitutive overexpression of cyclin D1, which can also be expressed (at a much lower level) by other B-cell lymphomas and is typically not detected in normal B lymphocytes. The overexpression of cyclin D1 leads to deregulation of the cell cycle at the G 1 /S phase transition: cyclin D1 binding to CDK4/6 activates the transcription factor E2F by phosphorylating its inhibitor, retinoblastoma 1 (RB1) and further promotes cyclin E/CDK2 activation, which triggers entry into the S phase of the cell cycle. Several secondary genomic alterations targeting genes involved in key molecular pathways have been reported as involved in MCL pathogenesis and/or its aggressive clinical course. Together these genetic alterations affect important pathways such as INK4Α/CDK4/RB1 and ARF/MDM2/p53 (cell cycle/survival), PI3K/AKT/mTOR (cell growth/survival), ataxia telangiectasia mutated ( ATM ) gene at 11q22-23 (genetic stability), mutations or deletions of TP53 / RB or deregulation of checkpoint kinases CHK1 and CHK2 (DNA damage response), amplifications/overexpression of BCL2 (cell death/fate), or constitutive activation of nuclear factor κB (cell survival). Many of these genomic alterations as well as complex karyotypes have also definite prognostic value in MCL. SOX11 (neuronal transcription factor of the high-mobility group) expression is typically associated with minimal somatic hypermutation and genetic instability and with worse outcome. On the opposite, SOX11-negative variants are typically associated with indolent behavior; such cases (10%–15% of MCL) present with high white blood cell count, splenomegaly, no or minimal nodal disease (ie, mimicking chronic lymphocytic leukemia [CLL] but negative for both CD23 and CD200). These cases derive from postgerminal center B cells, show hypermutated IGHV , low/no karyotype complexity, and longer survival with prolonged stable clinical course. Rarely, some of these indolent (SOX11-negative) MCL may “transform” into aggressive disease usually associated with 17p/ TP53 alterations.
The classical immunophenotype of MCL reflects a mature B-cell lymphoma (positive for CD19, CD20, CD22, CD79a, PAX5, and FMC7) with coexpression of CD5. MCL cells also show typically immunoglobulin M/D positivity with more frequent lambda expression over kappa (ratio 1:13) and are negative for CD23, CD10, CD200, and BCL6. The diagnosis is confirmed through cyclin D1 overexpression and/or by the presence of t(11;14) translocation, more frequently seen by fluorescence in situ hybridization than cytogenetics. A small subset of truly cyclin D1 -negative MCL (5%–10%) will show overexpression of cyclin D2 or D3 predominantly through alternative translocations with immunoglobulin light chain genes. SOX11 expression has been reported as a tool to help diagnose such cyclin D1-negative MCL, which otherwise cannot be distinguished by gene-expression profiling (GEP), and carry similar clinical characteristics and outcome and therefore should be treated accordingly.
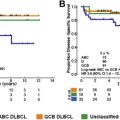
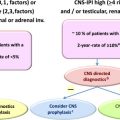
Typically, MCL patients present with advanced stage disease (>80% Ann Arbor stage IV), although B symptoms are found in less than one-third of patients. One remarkable feature of MCL is the almost constant extranodal involvement, including gastrointestinal tract, liver, and spleen, but also bone marrow and peripheral blood (flow peripheral blood lymphocyte positive in >90% cases). Recent reports suggest that central nervous system (CNS) involvement might be underestimated in MCL, although its incidence at baseline remains low (<1%), whereas CNS involvement can occur in up to 15% to 20% at 5 years, particularly in patients with high-risk disease, high Ki-67, and/or blastoid variants and carries then regardless a dismal prognosis.
Although treatment strategies in MCL have been very diverse, the persistent disappointing outcome led to explore novel approaches early on, which have translated over time into an improvement of patient outcome from a median overall survival (OS) of 2.5 years in the late 1970s to 4.8 years in the mid 1990s and well over 5 to 7 years in the late 2000s. Not surprisingly, this continued improvement is attributable to several factors from better supportive care to the use of dose-intensive (DIT)/high-dose therapies (HDT), which have clearly led to much longer progression-free survival (PFS) intervals, and the development of promising novel therapies for a disease that commonly shows chemoresistance in the relapse setting. Nevertheless, there remains nowadays a wide heterogeneity in the management of MCL, with many different treatment approaches, which may be influenced by age, comorbidities, disease biology, as well as patient and physician preferences. This is reflected by the rather long list of potential regimens (>10 options) for initial treatment of MCL in the National Comprehensive Cancer Network current guidelines. In itself, such diverse management definitely represents a true challenge, including a greater heterogeneity in the relapse setting, but looking at the overall picture, patterns emerge that might help clarify treatment options and shed some light on emerging trends and shifting paradigm.
Background
The field of mantle cell lymphoma (MCL) has changed dramatically since its recognition as a separate entity more than 30 years ago. The concept of mantle-zone lymphoma first introduced in 1982 by Weisenburger and colleagues was confirmed by the International Lymphoma Study Group in 1992 and refined in the Revised European-American Lymphoma and World Health Organization classification in 1994. MCL recognition was based on its distinct morphologic and molecular features (hallmark t(11;14) translocation), but also its immunophenotype and distinct clinical course, with much poorer outcome among “indolent lymphomas.”
MCL represents 6% to 10% of non-Hodgkin lymphomas with a median age at diagnosis in the mid to late 60s and a clear predominance in men (ratio 3:1). Some data suggest a possible increase in MCL incidence over the last two decades, albeit likely reflecting improved diagnostics. Although most MCL cases are thought to derive from an antigen-naive pre-germinal center B cell, there is definite evidence of cases with restricted immunoglobulin gene repertoire (particularly IGHV3-21 and IGHV4-34 genes), which together with precise somatic hypermutation patterns suggest a role for chronic antigenic stimulation. Moderate associations with MCL risk have been reported for Borrelia burgdorferi infection, lifestyle-related factors, family history of hematopoietic malignancies, or genetic susceptibility (interleukin-10 and tumor necrosis factor genes), while others suggest molecularly defined antigenic specificity for B-cell receptor (BCR) in some series.
The t(11;14)(q13;q32) translocation that juxtaposes the proto-oncogene CCND1 at 11q13 to the immunoglobulin heavy chain complex ( IGH ) at chromosome 14q32 is considered the primary oncogenic mechanism (although not sufficient) for the development of MCL. This translocation forces the constitutive overexpression of cyclin D1, which can also be expressed (at a much lower level) by other B-cell lymphomas and is typically not detected in normal B lymphocytes. The overexpression of cyclin D1 leads to deregulation of the cell cycle at the G 1 /S phase transition: cyclin D1 binding to CDK4/6 activates the transcription factor E2F by phosphorylating its inhibitor, retinoblastoma 1 (RB1) and further promotes cyclin E/CDK2 activation, which triggers entry into the S phase of the cell cycle. Several secondary genomic alterations targeting genes involved in key molecular pathways have been reported as involved in MCL pathogenesis and/or its aggressive clinical course. Together these genetic alterations affect important pathways such as INK4Α/CDK4/RB1 and ARF/MDM2/p53 (cell cycle/survival), PI3K/AKT/mTOR (cell growth/survival), ataxia telangiectasia mutated ( ATM ) gene at 11q22-23 (genetic stability), mutations or deletions of TP53 / RB or deregulation of checkpoint kinases CHK1 and CHK2 (DNA damage response), amplifications/overexpression of BCL2 (cell death/fate), or constitutive activation of nuclear factor κB (cell survival). Many of these genomic alterations as well as complex karyotypes have also definite prognostic value in MCL. SOX11 (neuronal transcription factor of the high-mobility group) expression is typically associated with minimal somatic hypermutation and genetic instability and with worse outcome. On the opposite, SOX11-negative variants are typically associated with indolent behavior; such cases (10%–15% of MCL) present with high white blood cell count, splenomegaly, no or minimal nodal disease (ie, mimicking chronic lymphocytic leukemia [CLL] but negative for both CD23 and CD200). These cases derive from postgerminal center B cells, show hypermutated IGHV , low/no karyotype complexity, and longer survival with prolonged stable clinical course. Rarely, some of these indolent (SOX11-negative) MCL may “transform” into aggressive disease usually associated with 17p/ TP53 alterations.
The classical immunophenotype of MCL reflects a mature B-cell lymphoma (positive for CD19, CD20, CD22, CD79a, PAX5, and FMC7) with coexpression of CD5. MCL cells also show typically immunoglobulin M/D positivity with more frequent lambda expression over kappa (ratio 1:13) and are negative for CD23, CD10, CD200, and BCL6. The diagnosis is confirmed through cyclin D1 overexpression and/or by the presence of t(11;14) translocation, more frequently seen by fluorescence in situ hybridization than cytogenetics. A small subset of truly cyclin D1 -negative MCL (5%–10%) will show overexpression of cyclin D2 or D3 predominantly through alternative translocations with immunoglobulin light chain genes. SOX11 expression has been reported as a tool to help diagnose such cyclin D1-negative MCL, which otherwise cannot be distinguished by gene-expression profiling (GEP), and carry similar clinical characteristics and outcome and therefore should be treated accordingly.
Typically, MCL patients present with advanced stage disease (>80% Ann Arbor stage IV), although B symptoms are found in less than one-third of patients. One remarkable feature of MCL is the almost constant extranodal involvement, including gastrointestinal tract, liver, and spleen, but also bone marrow and peripheral blood (flow peripheral blood lymphocyte positive in >90% cases). Recent reports suggest that central nervous system (CNS) involvement might be underestimated in MCL, although its incidence at baseline remains low (<1%), whereas CNS involvement can occur in up to 15% to 20% at 5 years, particularly in patients with high-risk disease, high Ki-67, and/or blastoid variants and carries then regardless a dismal prognosis.
Although treatment strategies in MCL have been very diverse, the persistent disappointing outcome led to explore novel approaches early on, which have translated over time into an improvement of patient outcome from a median overall survival (OS) of 2.5 years in the late 1970s to 4.8 years in the mid 1990s and well over 5 to 7 years in the late 2000s. Not surprisingly, this continued improvement is attributable to several factors from better supportive care to the use of dose-intensive (DIT)/high-dose therapies (HDT), which have clearly led to much longer progression-free survival (PFS) intervals, and the development of promising novel therapies for a disease that commonly shows chemoresistance in the relapse setting. Nevertheless, there remains nowadays a wide heterogeneity in the management of MCL, with many different treatment approaches, which may be influenced by age, comorbidities, disease biology, as well as patient and physician preferences. This is reflected by the rather long list of potential regimens (>10 options) for initial treatment of MCL in the National Comprehensive Cancer Network current guidelines. In itself, such diverse management definitely represents a true challenge, including a greater heterogeneity in the relapse setting, but looking at the overall picture, patterns emerge that might help clarify treatment options and shed some light on emerging trends and shifting paradigm.
From “more is better” to establishing new standards in the dose-intensive therapy/high-dose therapy settings
Based on the poor results of conventional chemotherapy regimens (CVP [cyclophosphamide, vincristine, and prednisolone], MCP [mitoxantrone, chlorambucil, and prednisolone], cyclophosphamide, doxorubicin, vincristine, and prednisolone [CHOP]) in MCL, a natural shift led to the use of HDT followed by autologous stem cell transplantation (ASCT) as consolidation in first remission. The initial favorable results of smaller phase II trials were confirmed by a large German phase III trial in which responding patients to CHOP chemotherapy were randomized between maintenance interferon (IFN-α) versus HDT-ASCT. In that study, there was a significant improvement of both PFS and duration of response (DOR) in favor of the HDT-ASCT consolidation arm (but no difference in OS likely due to crossover design) ( Table 1 ).
| Study for DIT-HDT-FIT Patients | Setting | No. of Patients | MIPI % (L/I/H) | ORR, % | CR, % | Med PFS | Med OS | Comments |
|---|---|---|---|---|---|---|---|---|
| R-CHOP-R-DHAP/ASCT Delarue 2013 | Ph II multicenter | 60 | 55/32/13 | 100 | 96 | 6.9 y | 5 y OS 75% | |
| R-Maxi-CHOP/HDAraC/ASCT (MCL NORDIC-2) (maint based on RQ PCR) Geisler 2008 | Ph II multicenter | 160 | 51/26/23 | 96 | 54 | 7.5 y | 10 y OS 64% | Mol relapses received additional R2 (not considered failures) |
| R-CHOP vs R-CHOP/R-DHAP/ASCT Hermine 2016 | Ph III multicenter | 497 | 60/25/15 | R-CHOP 90 | 83 | Med TTF 9 y vs 3.9 y | Exp arm also > for OS | Earlier and deeper CR and mol CR in exp arm R-CHOP/R-DHAP |
| R-CHOP/R-DHAP 95 | 82 | |||||||
| R-DHAP/ASCT/Maint R2 LeGouill 2014 | Ph III multicenter | 299 | 53/27/19 | NA | 92 | Med PFS 88% in maint arm vs 745 in Obs. arm | Maint q2 ms × 3 y MRD studies: pre-ASCT MRD status +++ impact on outcome R maint improves PFS regardless of MRD status pre-ASCT {Callanan, 2015 #118314} | |
| R-Maxi-CHOP/HDAraC/90Y-ibritumomab-tiuxetan/ASCT (MCL NORDIC-3) | Ph II multicenter | 160 | 48/31/21 | 97 | 67 | 4 y EFS 62% | 4 y OS 78% | RIT was given to non-CR pts after receiving similar induction than MCL2 |
| R-HyperCVAD Romaguera 2010 | Ph II single center | 97 | 47/29/18 | 97 | 87 | Med TTF for <65 y 6.9 y | NR | Estimated 15-y FFS of 30% in ≤65 y {Chihara, 2016 #118285} |
| R-HyperCVAD Bernstein 2013 | Ph II multicenter | 49 | 55/31/14 | 86 | 47 | Med PFS 4.8 y | 6.8 y | |
| R-HyperCVAD Merli 2011 | Ph II multicenter | 63 | 60/33/7 | 83 | 72 | 5 y PFS 61% | 5 y OS 73% |
| Study for Non DIT-HDT FIT Patients (ie, Elderly) | Setting | No. of Patients | MIPI % (L/I/H) | ORR, % | CR, % | Med PFS | Med OS | Comments |
|---|---|---|---|---|---|---|---|---|
| R-CHOP alone Lenz 2005 | Ph II multicenter | 62 | NA | 94 | 34 | Med TTF 21 ms | NA | |
| R-CHOP/B-R Rummel 2013 | Ph III multicenter | 274/275 | NA | 93 | 30 | Med PFS 35 ms vs 22 ms for R-CHOP | No diff | |
| B-R vs R-CHOP/R-CVP Flinn 2014 | Ph III multicenter | 36/38 | NA | 97/91 | 31/25 | NA (but no diff) | NR | |
| R-CHOP vs FCR Kluin-Nelemans 2012 | Ph III multicenter | 560 | NA | 86/78 | 34/40 | Med TTF 26/28 ms | 62/47 P = .005 | More toxicity and POD in FCR arm In responders to R-CHOP, maint R improved DOR and OS |
| R-BAC Visco 2013 | Ph II multicenter | 40 | 28/25/47 | 100 | 95 | 2 y PFS 95% | 95% | Study had ½ untreated and ½ r/r MCL |
| R-CHOP/90Y-ibritumomab-tiuxetan RIT Smith 2012 | Ph II multicenter | 56 | NA | 82 | 55 | Med TTF 34 ms | 5 y OS 73% | |
| R-CHOP-vs BTZ-R-CAP (LYM-3002) Robak 2015 | Ph III multicenter | 487 | 30/39/31 | 89/92 | 42/53 | Med PFS 14 ms vs 24 ms for VR-CAP P <.001 | 59% improvement PFS >CR rate >DOR of CR 18 ms vs 42 ms | |
| B-R with maintenance randomization (MAINTAIN) Rummel 2016 | Ph II multicenter | 122 | 16/45/37 | 85 | 27 | Med PFS 64 ms overall | NR | PFS obs 55 ms vs 72 ms in maint R arm P = .22 |
The next step was the addition of rituximab (Rtx) to established induction regimens for newly diagnosed MCL. In the ASCT setting, Rtx likely increased the transplantation eligible pool (improving response rate after induction) and helped as an in vivo purging before transplantation. The benefit of Rtx was also confirmed in the MCL2 Nordic Lymphoma Group trial (R-MaxiCHOP alternating with R-High-dose cytarabine followed by ASCT), which recent update showed a median event-free survival (EFS) >7 years. In this trial, patients were monitored for molecular relapse (not considered failures), which would trigger additional Rtx converting typically patients back into durable remission.
Several strategies, regrouped under DIT/HDT (see Table 1 ), have repeatedly confirmed an extension of the median PFS well over 5 years, comparing to rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP), which remains in the 14- to 18-months range. It became also clear through these DIT-HDT strategies that incorporating cytarabine as part of induction pre-ASCT was critical. The benefit of cytarabine, initially shown by a French group (R-CHOP-R-DHAP [rituximab plus dexamethasone, high-dose cytarabine, cisplatin]/ASCT, leading to tripled complete remission [CR] rate and a median EFS of 83 ms), was also a key conclusion of the NORDIC MCL2 trial mentioned above. The benefit of high-dose cytarabine was definitely proven thanks to a large and remarkable (>400 patients) EU phase III trial comparing R-CHOP/R-DHAP (alternating × 6) followed by HDT (using AraC Melphalan and total body irradiation [TBI]) versus R-CHOP × 6 followed by HDT (using Cy-TBI). The results showed superiority for the cytarabine-containing arm, in terms of time to treatment failure (TTTF), the primary endpoint, with a 30% reduction in the risk of progression but also superior OS ([NR] vs 82 ms, p .045); note, this advantage was seen across all MCL International Prognostic Index (MIPI) subgroups. These results were attributed to the quality of the response seen in the high-dose cytarabine arm with much earlier and higher CR rate than with R-CHOP, which translated into longer duration of first response and better outcome. In addition, built-in MRD studies in this study revealed the profound impact on outcome of achieving negative MRD status (ie, a molecular CR), which has now been shown to predict outcome across the board in several studies and will likely become a future key endpoint in MCL. In the randomized EU MCL trial, the molecular CR rate post induction was 83% in the cytarabine arm versus 51% in the control arm (p<.0001), confirming again the cytarabine arm superiority while translating into a new standard for DIT-HDT in MCL frontline therapy.
The induction for Nordic regimen MCL2 is not very different from R-HyperCVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone; alternating with methotrexate and high-dose cytarabine), another dose-intensive regimen frequently used in MCL patients 65 years or younger with MCL. The initial experience with R-HyperCVAD (97 patients; 1/3 >65 years old) showed a CR rate of 87% and a 3-year failure-free survival (FFS) of 73% in the 65 years and younger group, consistent with the results seen with ASCT consolidation. In a recent update with 15-year follow-up, the median OS exceeded 10 years for all patients, whereas about one-third of the 65 years and younger group were still in their first remission. Although the efficacy of R-HyperCVAD has been recognized in the multicenter setting, it is definitely associated with significant toxicity, including secondary MDS (although in smaller numbers than after HDT/ASCT), feeding the debate of benefit of intensive therapies in MCL. On the other hand, an abbreviated version (4 cycles) of R-HyperCVAD regimen has been used as induction pre-ASCT leading to very impressive results. On the other hand, based on the high CR (and molecular CR rate) seen with these high dose cytarabine containing regimens, one can logically wonder if HDT-ACST consolidation upfront is still needed. This issue is currently being addressed through the ongoing TRIANGLE study in Europe, which aims at introducing ibrutinib in the frontline setting, including a randomization of HDT-ASCT versus maintenance ibrutinib post induction. Another EU large (299 patients) phase 3 trial (LyMA) looked at R-DHAP x 4 cycles (and if not at least in PR, patients could receive 4 cycles of R-CHOP) followed by HDT-ASCT in untreated MCL (<66 years). Patients were randomized post-ASCT for observation versus Rtx maintenance (375 mg/m 2 every 2 months for 3 years). The CR/CRu rates before and after ASCT were 81% and 92%, respectively. At the last follow-up, the median EFS (primary endpoint) was not reached, and at 2 years was 93% in the Rtx arm versus 81% in the observation arm (hazard ratio 2.1). The study included again remarkable multicenter serial quantitative polymerase chain reaction (PCR) monitoring showing that pre-ASCT MRD status in both bone marrow (BM) and peripheral blood PB was a strong predictor of PFS in younger MCL patients. Early monitoring post-ASCT could help guide future MRD-based risk-adapted treatment. Interestingly, Rtx maintenance improved the PFS (ie, reduced the risk of recurrence) even in patients who were MRD negative post completion of induction-ASCT phase, suggesting potentially rare residual circulating or “tissue-resident” MCL cells.
The emergence of bendamustine in the management of elderly patients offered another opportunity as induction in younger patients as well. A randomized study of B-R (bendamustine + rituximab) against R-HyperCVAD in transplant-eligible patients was closed prematurely (53/160 patients accrued) due to unexpected (and surprising) failure of stem cell collection in the R-HyperCVAD arm. Of note in this trial, the CR rate post-R-HyperCVAD was very low (31%) versus 70% to 85% in other reported series. Nevertheless, results were encouraging with a 2-year PFS for R-Hyper-CVAD and B-R arms of 87% and 88%, respectively. In addition, in a subset of patients with MRD data available, results suggested that B-R can lead to deep remission with high-molecular CR rate. Although this needs to be validated in larger trials, B-R is also being looked at in combination with cytarabine (B-R/R-AraC induction) before ASCT with also preliminary but intriguing results. On the other hand, recent data suggest that cytarabine alone–based regimens might not be sufficient as frontline therapy for MCL.
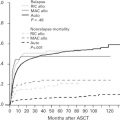
If no one would argue about the progress accomplished through DIT/HDT over standard therapy, such strategies are not always usable in MCL patients, given the median age at diagnosis in the mid to late 60s, although comorbidities, not just age, should be the critical factors for treatment decisions, as selected patients greater than 65 years can enjoy similar outcome as younger patients even with HDT-ASCT. However, such patients are typically excluded from studies, and it becomes then important to look at real world data outside clinical trials, where, unfortunately, overall the outcome of MCL has not really changed since the mid 1990s according to US registry data. However, even in that setting, interestingly, the impact of DIT/HDT has been verified. A large Scandinavian study of more than 1300 patients confirmed the positive impact of both Rtx-containing regimen and ASCT consolidation on MCL patients’ OS. In the United States, data from the SEER database comparing R-CHOP versus R-HyperCVAD or R-CHOP/R-HyperCVAD/ASCT confirmed in our experience, that R-CHOP leads to clearly inferior outcome than DIT-HDT strategies, both for PFS and for OS when comparing pooled DIT/HDT versus R-CHOP alone.
In summary
- •
DIT/HDT strategies lead to a much higher CR rate, in the range of 55%–80% pre-ACST and going up to 85% to 90% post-ACST (vs 30%–35% range for R-CHOP or 35%–45% for B-R alone), which not surprisingly translates into much more durable remission and disease-free intervals leading to OS advantage.
- •
Furthermore, induction regimens that incorporate Rtx and high-dose cytarabine lead to a very high rate of early molecular CR that is emerging as likely a critical endpoint and is currently being validated in ongoing MCL trials.
- •
Although there are limited data yet to compare with DIT, small phase II studies support further exploration of potentially less toxic regimens such as B-R or B-R + cytarabine as induction as well as in younger patients.
- •
To build on the success of DIT/HDT, ongoing studies are also looking at a combinations with novel agents together or as maintenance/consolidation post-HDT. Preliminary results of bortezomib as consolidation or maintenance post-HDT-ASCT (CALGB) suggests improved outcome compared with historical controls. Meanwhile, the benefit of maintenance Rtx was also shown after HDT as mentioned in the LyMa trial above, significantly reducing the risk of relapse and prolonging PFS. Although there was no OS advantage in the maintenance arm in that study, a combination of Rtx plus other biologicals might further improve the outcome post induction in MCL and is the subject of several ongoing clinical trials, including after HDT-ASCT.
Patients not eligible for dose-intensive therapy/high-dose therapy approaches: building up on new backbones, and impact of maintenance instead of consolidation with high-dose therapies/autologous stem cell transplantation
Given the median age at diagnosis (in some series up to 70 years), alternative approaches to DIT/HDT are needed. When added to CHOP, Rtx clearly increased overall response rate (ORR), CR rate, and TTTF but had no significant impact on PFS (25% at 2 years) or OS compared with CHOP alone. Although BR has been reported superior to R-CHOP (med PFS 22 vs 35 ms, p = .004) in the MCL subset (92 patients) from the STiL trial, the attempted confirmatory BRIGHT trial in the United States was not suggestive of superiority of BR over R-CHOP (except for CR rate, although control arm had pooled R-CHOP-R-COP [is CHOP without antracyclin]). Fludarabine-containing regimens such as fludarabine, cyclophosphamide and rituximab (FCR) had shown durable remission in MCL and was tested against R-CHOP in a large (560 patients) randomized trial in elderly MCL (>60 and/or not eligible for HDT). A second randomization in this trial looked at maintenance (until POD or toxicity) with Rtx versus IFN-α. Although the CR rate was similar (40% with FCR vs 34% with R-CHOP), both progressive disease and toxicity were worse with FCR as well as OS (47% with FCR vs 62% with R-CHOP, p = .005). Interestingly, looking at maintenance impact, Rtx reduced the risk of progression or death by 45% (4 years remission, 58%, vs 29% with IFN-α; p< .01). In addition, in patients responding to R-CHOP, R2 maintenance significantly improved OS (4-year OS 87%, vs 63% with IFN-α; P = .005). Putting aside any caveat from selection (related to double randomization design), such results are not very different from HDT/ASCT seen in younger patients, suggesting that maintenance might provide similar benefit as consolidation with ACST in some cases. Although the maintenance benefit has been shown in both younger (post-ASCT) and elderly patients, this might depend on the context, particularly on the type of induction as shown recently with the MAINTAIN trial of maintenance Rtx versus observation after B-R induction in non-ASCT candidates of MCL patients. Although this study might have been underpowered, similar results were seen in the EU trial FCR arm, where maintenance Rtx had no impact, suggesting that lymphopenia commonly seen after either fludarabine or bendamustine might interfere with effector cells responsible for most of Rtx effect.
The emergence of novel agents in the relapsed/refractory setting with nonoverlapping toxicities with cytotoxics offered an opportunity for new combinations. The recent LYM3002 phase III trial compared 6 cycles of R-CHOP versus R-CAP + bortezomib (1.3 mg/m 2 IV on days 1, 4, 8, and 11) in non-HDT/ASCT eligible newly diagnosed MCL patients (244 per arm), aiming at PFS as primary endpoint. After a median follow-up of 40 months, results showed a relative improvement of 59% of median PFS (by independent radiologic review) from 14.4 months in the R-CHOP group to 24.7 months in the VR-CAP group ( p <.001). Secondary end points were consistently improved in the VR-CAP group, including CR rate (42% vs 53%), median CR duration (18.0 months vs 42.1 months), median treatment-free interval (20.5 months vs 40.6 months), and 4-year OS rate (54% vs 64%). Rates of neutropenia and thrombocytopenia were higher in the VR-CAP group but manageable, setting a new standard and becoming the first US Food and Drug Administration (FDA) -approved frontline combination in MCL. Similarly, a modified R-HyperCVAD regimen (no methotrexate, no cytarabine, and built-in maintenance with 4 weekly doses of Rtx 375 mg/m 2 every 6 months for 2 years), to reduce toxicity, was initially piloted in previously untreated MCL and then combined with bortezomib (Vc-R-CVAD). Results showed a very promising ORR of 90% and CR rate of 77% (vs 77% and 63%, respectively, in modified R-HyperCVAD without bortezomib), translating into a 3-year PFS of 63% and OS of 86%. The benefit of this combination was confirmed in the extended Eastern Cooperative Oncology Group (ECOG)-1405 trial, with interestingly similar results in patients who received maintenance Rtx or underwent ASCT consolidation, which was optionally offered in this trial.
Despite the lack of difference in OS of BR versus R-CHOP, its favorable short-term toxicity profile, particularly in the STiL trial, established a new backbone in MCL for combinations, such as BR plus bortezomib, which showed very promising results in phase II studies in the relapsed/refractory setting (83% ORR, 52% CR). This concept is currently tested in the frontline setting in a large intergroup randomized US trial, which also integrates maintenance Rtx versus Rtx plus lenalidomide. The LYSA group recently presented impressive results with RiBVD (rituximab, bendamustine, bortezomib, and dexamethasone) in 74 frontline elderly MCL (no maintenance) with a 74% CR/CRu rate alongside measurable molecular remissions in peripheral blood (83%) and bone marrow (74%), translating into an estimated 24-month PFS and OS of 69% and 80%, respectively. Other combinations with BR are ongoing, such as with ibrutinib (SHINE randomized phase III trial in frontline >65 years MCL completed, results pending) or with other biologicals such lenalidomide, with promising CR rate (NORDIC MCL4 trial) or temsirolimus, in either combination or maintenance, including as part of the randomized evaluation between high-dose cytarabine containing regimen versus R-CHOP for elderly MCL patients. Finally, the addition of cytarabine to BR was reported in MCL patients 65 years of age or older; although a small series, results were impressive with 100% ORR (95% CR) and 95% 2-year PFS for previously untreated MCL (n = 20), and 80% ORR (74% CR) with a 70% 2-year PFS for relapsed/refractory (R/R) MCL (n = 20). With more novel agents in the pipeline, in the future, studies will likely aim at continuing to build up on such platforms, with the goal and hope to reach early on deeper responses as in younger patients, a critical factor toward better long-term disease control.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


