As we have highlighted in the other cases, the clinical management of catecholamine-secreting pheochromocytomas or paragangliomas (PPGLs) can be challenging—both diagnostically and therapeutically. However, when PPGL is diagnosed in the setting of pregnancy, the complexity rises more than 10-fold. Herein we share a case of a patient in whom recurrent and malignant pheochromocytoma was diagnosed during pregnancy.
Case Report
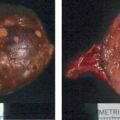
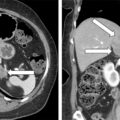
This 28-year-old woman was referred to Mayo Clinic during her 13th week of pregnancy for recurrent and malignant pheochromocytoma. She was first seen at Mayo Clinic 8 years previously (at 20 years of age) when she presented with a 1-year history of recurrent paroxysms of nausea, vomiting, headaches, and palpitations. The symptoms proved to be due to a right adrenal pheochromocytoma. The preoperative plasma normetanephrine was 21.2 nmol/L (normal, <0.9) and plasma metanephrine was 18.7 nmol/L (normal, <0.5). The abdominal computed tomography (CT) scan showed a heterogeneous necrotic 6.5-cm right adrenal mass ( Fig. 94.1 ). At open laparotomy the 7.3 × 7.8 × 4.9–cm right adrenal pheochromocytoma was resected without complication or tumor capsule violation ( Fig. 94.2 ). The postoperative plasma fractionated metanephrine levels were normal. Germline genetic testing was discussed, and the patient declined to pursue because of lack of insurance coverage. She had annual biochemical testing to screen for recurrent pheochromocytoma, and it was normal until her last test, which was done 2 years before the current consultation. Spells started 6 months before the current presentation—she would wake in the morning with a sense of a rush, pounding in her chest, and “internal shakiness” that would last 5–10 minutes. These symptoms became more marked and frequent after she became pregnant 13 weeks ago. Her only medication was a prenatal vitamin. On physical examination her BMI was 22.1 kg/m 2 , blood pressure 115/72 mmHg, and heart rate 77 beats per minute. The retinal examination was normal, and no Lisch nodules were evident on examination of the iris bilaterally. The thyroid gland was normal to palpation. Examination of the skin was normal with absence of café au lait spots, axillary or inguinal freckling, and subcutaneous neurofibromas.


INVESTIGATIONS
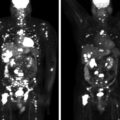
Laboratory studies at Mayo Clinic were diagnostic for an adrenergic catecholamine-secreting tumor ( Table 94.1 ). Magnetic resonance imaging (MRI) of the abdomen without gadolinium showed a soft tissue mass (2.7 cm × 6.3 cm × 5.7 cm) in the retrocaval retroperitoneum in the right adrenalectomy bed ( Fig. 94.3 ).
| Gestational Week | |||||
| Biochemical Test | 13 Weeks | 19 Weeks | 30 Weeks | 6 Weeks Postpartum | Reference Range |
| Sodium, mmol/L Potassium, mmol/L Creatinine, mg/dL Plasma metanephrine, nmol/L Plasma normetanephrine, nmol/L 24-Hour urine: Metanephrine, mcg Normetanephrine, mcg | 138 4.4 0.6 10 5.3 5356 1450 | 8.1 4.8 | 18 7.0 | 13 8.6 | 135–145 3.6–5.2 0.59–1.04 <0.5 <0.9 <400 <900 |
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Lynch Syndrome
Adrenocortical Carcinoma Associated With Lynch Syndrome
 Metastatic Paraganglioma: Role for Systemic Chemotherapy
Metastatic Paraganglioma: Role for Systemic Chemotherapy
 Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
Cushing Syndrome Associated With Ectopic Corticotropin and Corticotropin-Releasing Hormone–Secreting Pheochromocytoma
 Bilateral Macronodular Adrenal Hyperplasia in the Setting of Multiple Endocrine Neoplasia Type 1
Bilateral Macronodular Adrenal Hyperplasia in the Setting of Multiple Endocrine Neoplasia Type 1
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


