FIGURE 21.1 Three orders of ramification of the proper hepatic artery are shown color coded. First order (red) is division into right (A) and left (B) hepatic arteries. The second order is division into sectional arteries (green), including the right anterior (c), the right posterior (d), the left medial (e), and the left lateral (f) sectional arteries. The third-order division (blue) is into segmental arteries that are numbered and correspond to the Couinaud segments. The three orders supply the hemilivers or livers, sections, and segments. Note that the second order and third order for the left medial sectional artery and artery to segment 4 are identical (banded green and blue). Segment 1, which is separate from the two hemilivers, is supplied by the arteries that arise from the right and left hepatic arteries (not shown). Ramification of the bile ducts is identical to that of the arteries. (From Strasberg SM, Philips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg 2013;257(3):377–382.)
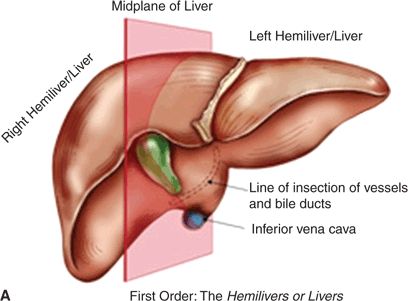
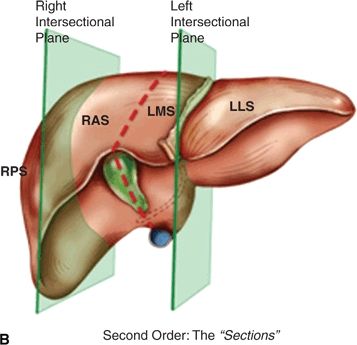
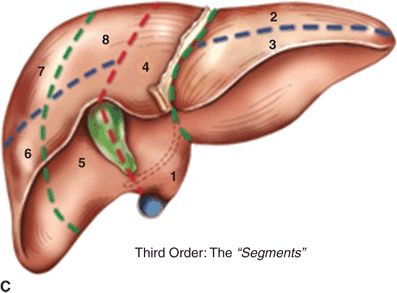
FIGURE 21.2 A. First-order division of the liver into the hemilivers or livers. Midplane of the liver shown in red. B. Second-order division of the liver into sections. (RPS, right posterior section; RAS, right anterior section; LMS, left medial section; LLL, left lateral section.) The intersectional planes are shown in green. C. Third-order division into numbered segments. (From Strasberg SM, Philips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg 2013;257(3):377–382.)
The second-order branches (Figs. 21.1 and 21.2) of the hepatic artery supply the four hepatic sections. The right liver has two sections, the right anterior section and the right posterior section, supplied by the right anterior sectional hepatic artery and the right posterior sectional hepatic artery, respectively (Fig. 21.1). The plane between these sections is the right intersectional plane, which does not have surface markings to indicate its position (Fig. 21.2). The left liver also has two sections, the left medial section and the left lateral section, which are supplied by the left medial sectional hepatic artery and the left lateral sectional hepatic artery (Fig. 21.1). The plane between these sections is referred to as the left intersectional plane. It does have surface markings indicating its position—the umbilical fissure and the line of attachment of the falciform ligament to the anterior surface of the liver.
The third-order branches of the hepatic artery divide the right and left hemilivers into segments 2 to 8 (Figs. 21.1 and 21.2). Each of the segments has its own feeding segmental artery. The left lateral section is divided into Sg2 and Sg3. The pattern or ramification of vessels within the left medial section does not permit subdivision of this section into segments, each with its own arterial blood supply. Therefore, the left medial section and Sg4 are synonymous. However, segment 4 is arbitrarily divided into superior (4a) and inferior (4b) parts. The right anterior section is divided into two segments, Sg5 and Sg8. The right posterior section is divided into Sg6 and Sg7. The planes between segments are referred to as intersegmental planes. The ramifications of the bile ducts are identical to that described for the arteries as are the zones of the liver drained by their respective ducts.
Segment 1 (caudate lobe) is a distinct portion of the liver, separate from the right and left hemilivers. It has three parts: the bulbous left part (spigelian lobe); the paracaval portion, which lies anterior to the vena cava; and the caudate process (or right part), on the right (Fig. 21.3). The caudate lobe is situated posterior to the hilum and the portal veins. The caudate receives vascular supply from both right and left hepatic arteries (and portal veins). Caudate bile ducts drain into both the right and left hepatic ducts. The caudate lobe is drained by several short caudate veins that enter the IVC directly. These veins enter the IVC on either side of the midplane of the vessel, an anatomical feature that normally allows the creation of a tunnel behind the liver on the surface of the IVC without encountering the caudate veins.
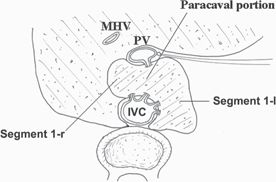
FIGURE 21.3 Anatomy of caudate lobe. Segment 1-1, caudate lobe proper; Segment 1-r, caudate process; MHV, middle hepatic vein; PV, portal vein; IVC, inferior vena cava
Resectional Terminology
Anatomic liver resections are hemihepatectomies (or hepatectomies), sectionectomies, or segmentectomies. The nomenclature for specific resections is described in Figures 21.4 to 21.8.
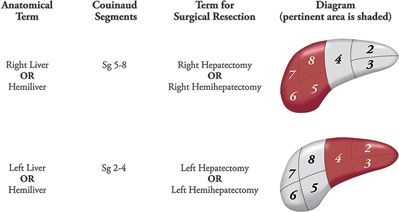
FIGURE 21.4 Resectional terminology for excision of a hemiliver or liver. (From Strasberg SM, Philips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg 2013;257(3):377–382.)
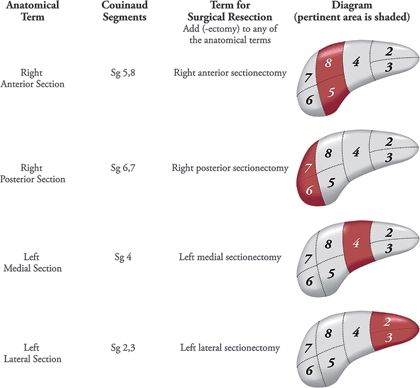
FIGURE 21.5 Resectional terminology for excision of a section. (From Strasberg SM, Philips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg 2013;257(3):377–382.)
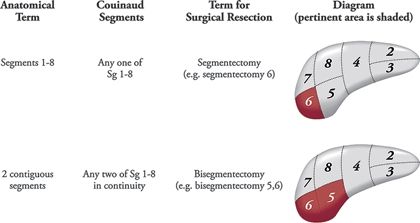
FIGURE 21.6 Resectional terminology for excision of a segment. (From Strasberg SM, Philips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg 2013;257(3):377–382.)
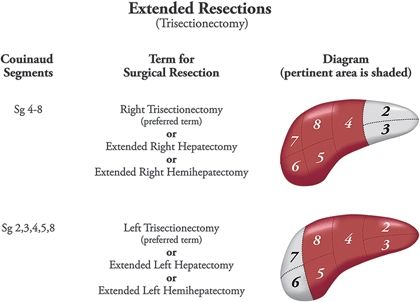
FIGURE 21.7 Terminology for extended resections (three sections). (From Strasberg SM, Philips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg 2013;257(3):377–382.)
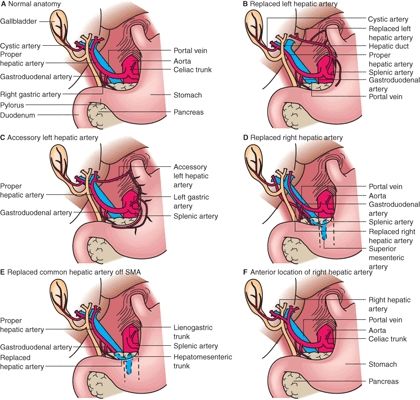
FIGURE 21.8 Prevailing pattern (“normal anatomy”) and some common variations of the hepatic artery. (From Mulholland MW, Lillemoe KD, Doherty GM, et al. Greenfield’s surgery: scientific principles & practice, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.)
Resection of segment 1 is usually called a caudate lobectomy.
SURGICAL ANATOMY FOR LIVER RESECTIONS
Hepatic Arteries and Liver Resections
In the prevailing anatomic pattern, the celiac artery terminates by dividing into splenic and common hepatic arteries. The common hepatic artery runs anteriorly and to the right to ramify into gastroduodenal and proper hepatic arteries. The proper hepatic artery enters the hepatoduodenal ligament and normally runs for 2 to 3 cm along the left side of the common bile duct (CBD) and terminates by dividing into the right and left hepatic arteries, the right immediately passing behind the common hepatic duct (CHD). The four sectional arteries arise from the right and left arteries 1 to 2 cm from the liver. Variations from this pattern, such as replaced (aberrant) arteries, are common. “Replaced” means that the artery supplying a particular volume of the liver is in an unusual location and also that it is the sole supply to that volume of the liver. This should not be confused with the term “accessory” artery. Accessory in this sense indicates that the artery is not the sole blood supply to an area (Fig. 21.8).
Part or all of the liver is supplied by a replaced artery in 25% of patients. The replaced right hepatic artery arises from the superior mesenteric artery (SMA) and usually runs behind and then along the right posterior border of the CBD (Fig. 21.8), where it may often be palpated. It may supply a segment of, a section of, or the entire right hemiliver. The replaced left hepatic artery arises from the left gastric artery and courses in the lesser omentum to the liver. Rarely, a replaced artery supplies the entire liver, and then it is called a replaced common hepatic artery.
Bile Ducts and Liver Resections
The prevailing pattern of bile duct drainage from the right liver is shown in (Fig. 21.9A). There are important biliary anomalies on the right side of the liver. The right posterior sectional duct inserts into the left hepatic duct in 20% of persons (Fig. 21.9B), and the right anterior bile duct does so in 6% (Fig. 21.9C). A right sectional bile duct inserting into the left hepatic duct is in danger of injury during left hepatectomy. Another important anomaly is insertion of a right bile duct into the biliary tree at a lower level than the prevailing site of confluence (Fig. 21.9D). The latter anomaly places the aberrant duct at great risk for injury during laparoscopic cholecystectomy.
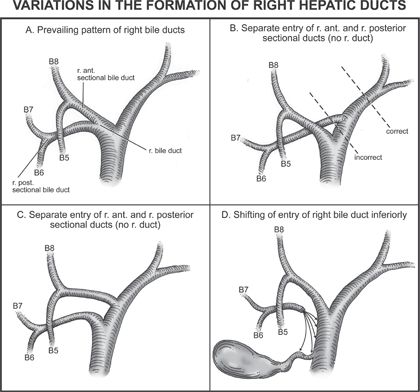
FIGURE 21.9 Prevailing pattern and important variations of bile ducts draining the right hemiliver. (From Fischer JE, Jones DB, Pomposelli FB, et al. Fischer’s mastery of surgery, 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2011.)
The prevailing pattern of bile duct drainage from the left liver and common anomalies is shown in Figure 21.10.
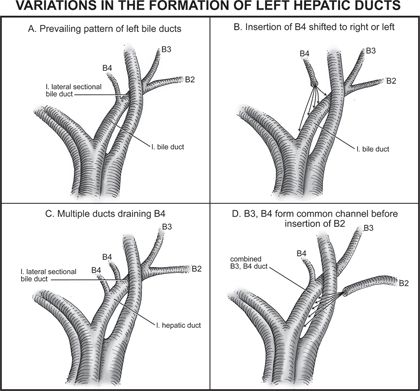
FIGURE 21.10 Prevailing pattern and important variations of bile ducts draining the left hemiliver. (From Fischer JE, Jones DB, Pomposelli FB, et al. Fischer’s mastery of surgery, 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2011.)
Portal Veins and Liver Resections
On the right side of the liver, the portal vein divisions correspond to those of the hepatic artery and bile duct, and they supply the same hepatic volumes (Fig. 21.11). It divides into two sectional and four segmental veins as do the arteries and bile ducts. The left portal vein consists of a horizontal or transverse portion, which is located under Sg4, and a vertical part or umbilical portion, which is situated in the umbilical fissure (Fig. 21.11
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


