Allogeneic hematopoietic cell transplantation (HCT) provides curative therapy for a variety of diseases. Over the past several decades, significant advances have been made in the field of HCT, and now HCT has become an integral part of treatment modality for a variety of hematologic malignancies and nonmalignant diseases. Historically, the limitation of HCT has been transplant-related mortality (TRM). In order to offer the curative HCT treatment option to most patients, safer regimens with acceptable graft-versus-host-disease (GVHD)-associated morbidity and TRM are preferred. The development of less toxic pretransplant conditioning regimens, more effective prophylaxis of GVHD, improved infection control, and other advances in transplant technology have resulted in a rapidly growing number of transplant recipients surviving long-term free of the disease for which they were transplanted.1, 2
Since its introduction in the early 1970s the number of patients who undergo HCT for a variety of malignant and nonmalignant disorders has increased steadily and, today, nearly 60,000 allogeneic HCT are performed worldwide annually,1, 3, 4, 5 a number that has been increasing yearly. With broadening indications, more options for HCT, and improvement in survival, by 2020 there may be up to half a million long-term survivors after allogeneic HCT worldwide.6 In this era, a stem cell source can be found for virtually all patients who have an indication to receive HCT. Since 2007, more allo-HCT procedures have been performed using alternative donor stem cell sources, such as volunteer unrelated donors (URD) or cord blood, than related donors.5, 7 Haploidentical-related donor or cord blood transplantations (CBT) have emerged as alternatives to fill the gap for those patients who do not have matched related donors or URD, and the outcome of these types of transplantations are expected to be better than chemotherapy alone or even better than autologous-SCT for selected indications. All these result in a steady increase in numbers of long-term survivors after HCT, creating an enlarging pool of children, youth, and mature adults at risk for long-term complications of HCT.
Many patients who recover from immediate posttransplant problems eventually regain health and return to normal activities of life. For those who survive 2 or more years post-HCT, the prospect for long-term survival is excellent (85% at 10 years after HCT). Yet, among long-term survivors, mortality rates are 4- to 9-fold higher than observed in an age-adjusted general population for at least 30 years after HCT, yielding an estimated 30% lower life expectancy compared with someone who has not been transplanted.8 The most common causes of excess death other than recurrent malignancy are chronic GVHD (cGVHD), infections, second malignancies, respiratory diseases, and cardiovascular diseases (CVDs).3, 6, 8, 9, 10
cGVHD is a multisystem chronic alloimmune and autoimmune disorder that occurs later after HCT. It is characterized by immune dysregulation, decreased organ function, significant morbidity, and impaired survival. Approximately 10% to 30% of patients require continued immunosuppressive treatment because of cGVHD beyond 5 years after HCT.8, 11 Therefore, it is not surprising that cGVHD, corticosteroid, and other immunosuppressive therapies are major contributors to late complications after HCT.
With survivorship, a shift in survivorship care occurs from large transplant centers to community health care providers. As a result, many hematologists/oncologists and primary care physicians are assuming the post-HCT care of late effects. Preventive measures as well as early detection and treatment are important aspects to reducing morbidity and mortality. This chapter focuses on the essentials of diagnosis, screening, treatment, and long-term surveillance of survivors after HCT.
CARDIOVASCULAR EVENTS AND METABOLIC SYNDROME
CV causes are not only the leading contributor to mortality in the general population but also impact the health of long-term transplant survivors.12 CV morbidity and mortality is typically latent in the early survivorship period because of the younger age and superior performance of transplant candidates. Nevertheless, there is growing data suggesting that traditional CV risk factors are elevated in long-term survivors, and that risk factor elevation is persistent and eventually results in premature CV events. CVD manifests as coronary artery disease/events, cerebrovascular disease/events, or peripheral vascular disease/events. Susceptible patients need to be identified early, and screened for modifiable risk factors with early intervention where possible.
Cardiovascular Events
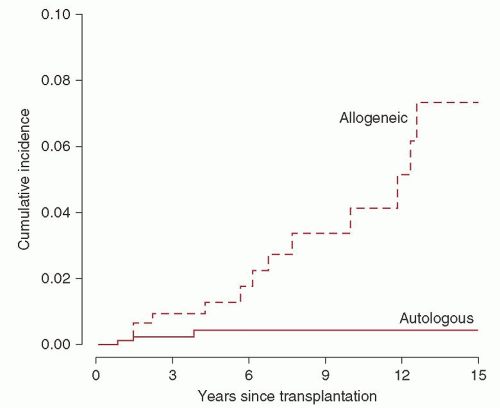
Tichelli et al. were the first to show that CV events occurred prematurely in transplant survivors (median age 49 years), albeit at a long interval after transplantation, with the cumulative incidence of late CVD being 22% at 25 years (Fig. 106.1).13 Interestingly, allogeneic HCT recipients were significantly more likely to have arterial events than autologous transplant recipients. The Late Effects Working Group of the European Group for Blood and Marrow Transplantation (EBMT) found a cumulative CV event incidence of 6% at 15 years.9 In a matched cohort study of 1,491 long-term survivors, transplant recipients experienced increased CV mortality (adjusted incidence rate difference, 3.6 per 1,000 person-years; 95% CI, 1.7 to 5.5) with increased cumulative incidence of ischemic heart disease, cardiomyopathy or heart failure, stroke, vascular diseases, and rhythm disorders.14
FIGURE 106.1. The cumulative incidence of cardiovascular events at 15 years, adjusted for age. (From Tichelli A, Bucher C, Rovo A, et al. Premature cardiovascular disease after allogeneic hematopoietic stem cell transplantation. Blood 2007;110:3463-3471.)
Disease Spectrum
Coronary artery disease and/or CV accidents are much more common than isolated peripheral artery disease. In a case control study of 63 patients with late CV disease, 44 subjects had coronary artery disease, and 19 had cerebrovascular diseases. Thirty-four of these 63 patients with CVD died, 31% of them from a CV event.15 Furthermore, CVD may contribute to chronic ill health seen in long-term survivors. The magnitude of chronic illness in a study of 1,022 HCT survivors was 59% at 10 years after HCT and increased in comparison to their sibling controls.16
Cardiovascular Risk Factors
Traditional CV risk factors include male gender, family history, dyslipidemia, diabetes mellitus, obesity, hypertension, chronic kidney disease (CKD), and smoking. In addition, transplant survivors have unique risk factors such as exposure to ionizing radiation, immunosuppressant use (including steroids), and endocrinopathies.
CV risk factors generally increase with age and it is difficult to attribute the emergence of new CV risk factors to the transplant process itself without a good control population. A clear increase in the incidence of diabetes and hypertension was seen in a study of 1,022 HCT survivors, with the incidence of CVD being 3-fold that of their sibling controls.16 In a cross-sectional study, HCT survivors had a 2.2-fold increase in the prevalence of metabolic syndrome, a clustering of CV risk factors characterized by abdominal obesity, dyslipidemia, hypertension, and elevated fasting glucose, compared to age- and gender-matched controls.17 In a long-term study (17.5 years median) of 44 pairs of recipients and their respective donors after HCT, recipients were more likely to have hypertension (P = 0.015), dyslipidemia (P = 0.002), lower glomerular filtration rates (GFRs) (P < 0.0001) and reduced thyroid function (P = 0.002).18 The occurrence of dyslipidemia is a function of age and immunosuppressive treatment. Dyslipidemia appears to play a central role in the elevated CVD risk after HCT.19 De novo dyslipidemias may even impact a pediatric population.20
Pathobiology
The factors leading to persistent elevation of CV risk in HCT survivors long after cessation of immunosuppression remain unclear. Residual effects from radiation, endocrine dysfunction (including steroid exposure, hypogonadism, hypothyroidism, and growth hormone deficiency), and endothelial damage have been implicated.
Chest irradiation is a validated cause of CV mortality. Extrapolating from the CV impact of chest irradiation in nontransplant populations with malignancy, it is reasonable to suspect that the use of total body irradiation (TBI) in transplant conditioning contributes to increased CVD risk, but this remains to be proven in a well-controlled study. Pretransplant chest radiation exposure was associated with a 9.5-fold higher risk of CVD.15
Hypothyroidism is a frequent late effect in transplant survivors and is related to conditioning with TBI and prolonged cGVHD.21 Hypothyroidism may affect ˜30% to 40% of survivors, is often subclinical in presentation, and is strongly linked to dyslipidemias. Gonadal dysfunction will occur in the majority of transplant survivors and is linked to conditioning intensity and recipient age. Endocrinopathy and metabolic syndrome are strongly associated with gonadal dysfunction.22 In males, metabolic syndrome and low androgen levels are strongly correlated,23 and in females, estrogens are necessary for maintenance of CV health.24, 25 In a series of 109 long-term allogeneic HCT survivors, CV risk factors were significantly elevated in males but not in females who were all recipients of hormonal supplementation.26 Relative growth hormone deficiency may be a factor in adult and pediatric transplant survivors. Growth hormone deficiency in adults leads to insulin resistance and is characterized by dyslipidemias and hypertension.27 Pediatric survivors of cancer treatment and HCT are particularly sensitive to the metabolic consequences of impaired growth hormone secretion.22, 28
Leptin is an adipokine responsible for regulating food intake and energy metabolism. Hyperleptinemia has been implicated as the pathobiologic link between transplant and metabolic syndrome.29, 30 Vascular endothelium may be the target of damage by radiation exposure and by alloreactivity (e.g., GVHD). Radiation has a dose-dependent impact on vasculature and endothelium in animal models. In a rodent model, TBI with 10 Gy injured coronary microvasculature, and altered endothelial physiology and myocardial mechanics.31 Host endothelial cells are a target of alloreactive donor cytotoxic T lymphocytes, and chronic skin GVHD is characterized by the progressive loss of microvessels.32 cGVHD is also characterized by elevations in von Willebrand factor,18 which may be released by endothelial injury. Chronic hypomagnesemia is common early after transplantation33 and is known to induce insulin resistance, diabetes, and metabolic syndrome. However, its precise impact on CV risk, if any, requires confirmation.
Management of Cardiovascular Risk
Since the burden of CV risk in transplant survivors has been poorly defined till now and CV events occur late, management of CV risk has often been a low priority. In a recent cross-sectional study of 86 adult survivors at a median of 3 years from HCT, 25% of cases with hypertension, 17% with abnormal glucose metabolism, and 60% with dyslipidemia were untreated.17 Current guidelines suggest a central role for transplantation centers in counseling primary health providers on screening and prevention.34
The management focus should be on modifiable CV risk factors: lifestyle (diet, smoking, and activity), obesity, diabetes, dyslipidemias, hypertension, hypothyroidism, hypogonadism, and other endocrinopathy. Dyslipidemias may be the most important driver of CV risk and are susceptible to therapy.26 The management of CV risk in transplant survivors is an evolving effort, but expert guidelines are now available.6, 12, 19Table 106.1 summarizes the approach to the hyperlipidemia in long-term survivors after HCT.
SECONDARY MALIGNANCIES
The risk of second malignancies as an important late effect after HCT was first recognized in the early 1990s. As the age and life expectancy of survivors continue to rise, second malignancies are expected to become an increasingly common complication.3
Secondary malignancies following HCT are commonly categorized into one of three histologic types: leukemia, lymphoma, and solid tumors.35 However, these disorders have distinctive chronology. Secondary leukemia generally occurs at a median of 6.7 months after auto-SCT, lymphoma at a median of 2.5 months, while the median time to development of solid tumors lies between 5 and 6 years.3
Risk of Second Malignancies and Risk Factors
Based on large retrospective analyses, the cumulative incidence of solid tumors following HCT ranges between 1.2% and 1.6% at 5 years, 2.2% and 6.1% at 10 years, and from 3.8% to 14.9% at 15 years post-HCT.36, 37, 38, 39 The incidence rate does not plateau; rather, there is a steady increase over time.39 Second cancers are a very important contributor to late nonrelapse mortality (NRM) in patients who survive more than 2 to 5 years posttransplantation, accounting for 5% to 10% of such deaths.8, 40, 41 And, in a recent study of 28,874 HCT survivors, the incidence of new solid tumors was double that of an age- and gender-matched general population.39 The risk increased over time, reaching 3-fold among patients followed for 15 years or more after transplantation.
TABLE 106.1 APPROACH TO LIPID MANAGEMENT IN HCT PATIENTS
Evaluation
Obtain fasting lipid profile prior to transplantation
Evaluate CVD Risk
1.
If patient has CVD or CVD risk equivalent, then manage as high-risk with appropriate therapy to reach LDL goal
a. Option to consider allogeneic HCT patients age 40 or older as high-risk
2.
Otherwise, calculate 10-y risk with online risk assessment tool (www.nhlbi.nih.gov) and manage LDL per ATP-III Guidelines
Monitor lipid profiles after HCT
1.
Check lipid profile within 4 wk after HCT then at least every 3 mo for patients on IST
2.
For patients at treatment goal on stable therapy every 6-12 mo as indicated, or after significant change in IST regimen in patients with dyslipidemia
3.
If patients develop significant dyslipidemia after HCT compared to baseline, consider secondary causes of dyslipidemia (IST, diabetes, hypothyroidism)
4.
Even patients without dyslipidemia should have lipids monitored every 1-2 y after allogeneic HCT, given increased CV risk
Management
If patient has high CVD risk (>20% 10-y risk), treat dyslipidemia with appropriate agent(s) to meet LDL goal, but monitor clinically if on IST or renal dysfunction
In patients with low (<10%)or moderate CVD risk (10-20%), consider drug treatment based upon severity of dyslipidemia, estimated prognosis post-HCT, and risks of lipid drug therapy (if on long-term IST for GVHD)
1.
Patients with low CVD risk that develop moderate secondary dyslipidemia on IST can be managed conservatively, if IST will be tapered off
2.
Patients with low to moderate CVD risk that develop severe hypertriglyceridemia (>500 mg/dl) should be treated to prevent pancreatitis
Consider referral to a lipid specialist for the following:
1.
Severe dyslipidemia (total cholesterol > 300 or LDL > 180, triglycerides > 500-1,000)
2.
Patients with dyslipidemia refractory to treatment and not meeting goals
3.
Patients with intolerance or contraindications to lipid lowering therapy
4.
Patients requiring combination lipid therapy, particularly in setting of IST
5.
Patients needing individualized CV risk assessment due to strong family history of premature CVD or other factors
The process of malignant transformation of secondary solid tumors after HCT is not well understood but multiple factors have been implicated.42 These include exposure to TBI, primary disease, male sex, and pretransplantation therapy. The risk of developing a nonsquamous cell cancer (SCC) is associated with younger age at transplantation and the use of radiation in the conditioning regimen. Radiation is also a known significant risk factor for the development of several other solid tumors, particularly cancers of the breast, thyroid, brain, central nervous system, bone and connective tissue, and melanoma; and screening is available for some of these tumors.10, 42 For the majority of these sites, risks are greater among those who survived 5 or more years after initial radiotherapy, in keeping with the latent period typical for radiation-related solid cancers.8, 10, 40, 43
cGVHD and immunosuppressive therapy (IST) are associated with SCC of the skin and mucosa.43, 44, 45 A particularly high-risk was observed in the 1 to 4 year interval after HCT, which remained elevated among long-term survivors. Duration of IST, and particularly prolonged exposure to azathioprine, has been associated with development of SCC.46
Several oncogenic types of human papillomavirus (HPV) have been implicated in the etiology of SCC of the female genital tract and head and neck, and may play a role in HCT-associated SCC.46, 47 Certainly, some inherited genetic polymorphisms have been reported to increase the risk of malignancies in patients who received alkylating agents either as pretransplant chemotherapy or as part of the conditioning regimen.48
Types of Secondary Solid Cancers
In a 2009 registry data study, 189 new cancers were found in 28,874 HCT recipients who underwent long-term follow-up.39 The average age at HCT was 27 years, and 67% received TBI as part of their conditioning regimen. The findings demonstrated that the risk of developing a nonSCC was dependent on the age at exposure to conditioning radiation. The relative risk of nonSCC for patients irradiated at ages <30 years was 9-fold that of nonirradiated patients, while the comparable risk for older patients was 1.1. cGVHD and male gender were the main determinants for the risk of SCC. The oral cavity, salivary glands, liver (prior hepatitis C exposure), skin, brain, breast, thyroid, and bone/connective tissue were the sites with a significant increase in secondary malignancy. These data indicate that HCT survivors, particularly those irradiated at young ages, face increased risks of solid cancers, supporting strategies to promote lifelong surveillance among these patients.
The risks of secondary solid cancers in HCT survivors who have not received irradiation are not well understood and deserve further study, because radiation-free conditioning regimens are being more frequently utilized. When chemotherapy alone is used for conditioning, the rates of solid tumors are still increased, as evidenced by a report examining solid tumor incidence in survivors who underwent high-dose busulfan-cyclophosphamide conditioning. In this study of 4,318 patients who received HCT for AML and CML, the cumulative incidence of solid tumors at 5 and 10 years after HCT was 0.6% and 1.2% for AML, and 0.9% and 2.4% for CML patients. The recipients had invasive solid cancers at a rate that was 1.4 times higher than expected in the general population.49 Sites with a significant increase in secondary malignancy included the oral cavity, esophagus, lung, soft tissue, and brain. cGVHD was found to be an independent risk factor for all solid cancers. Recipients of HCT using busulfancyclophosphamide conditioning are thus similar to TBI in the risk for developing solid cancers.
Diagnosis, Screening, and Prevention
Since there is no plateau in the incidence curve of new malignancies, consensus guidelines call for lifelong surveillance, and early diagnosis and treatment.50 Recommendations include the following: A. Recognition that radiation exposure and photosensitization by transplant medications increases the risk of skin malignancy, suggesting that survivors should protect against UV skin exposure by appropriate clothing or high-SPF sunscreen. B. Survivors should be reminded of the risks of secondary malignancies annually. Routine self-screening by breast and skin examination is to be encouraged, as is avoidance of high-risk behaviors, particularly all forms of tobacco use and unprotected UV exposure. C. Annual health screening should include symptom review for secondary malignancies. Screening mammography is recommended earlier than age 40 years for women exposed to radiation. Mucocutaneous involvement by GVHD increases the risk of malignant sequelae, and annual specialist examination (dermatologic, gynecologic, dental, or ENT) may be required.
Management
Successful management of second malignancies requires recognition of the special attributes of transplant survivors and close collaboration between the transplant center and the primary physician. Impaired hematopoietic reserve may be evident years after HCT and may manifest as prolonged myelosuppression after standard doses of cytotoxic agents or XRT. cGVHD management will often be a great challenge to treatment. Secondary SCC is biologically more aggressive, with frequent invasion beyond free surgical resection margins and metastasis to draining lymph nodes. Support should be provided for psychologic vulnerability in survivors facing a new diagnosis of malignancy.
LATE PULMONARY COMPLICATIONS
Lung injury is a frequent contributor to post-HCT morbidity and mortality.11, 51, 52 Pulmonary injury can be delayed, and the cumulative incidence of chronic pulmonary dysfunction in long-term HCT survivors ranges from 30% to 60%, depending on donor source and elapsed time from transplantation.11, 51 Bronchiolitis obliterans syndrome (BOS) is the most frequent and potentially lethal noninfectious pulmonary complication. BOS is now considered one of the diagnostic criteria for defining cGVHD by the NIH consensus report.52, 53 It is characterized by an insidious onset, high morbidity and mortality, and is typically accompanied by other manifestations of cGVHD. Much knowledge of BOS has been borrowed from the field of lung transplantation, in which BOS impacts more than half of the long-term survivors and is the major contributor to morbidity and mortality.54
Pathophysiology
Airway narrowing in BOS is mostly in the small airways, the terminal and respiratory bronchioles, with an internal diameter <2 mm. These small airways can be considered parallel highresistance conduits which account for the vast majority of the total airway volume and the cross-sectional area. Small airway damage must be extensive and 45% of the terminal bronchioles need to be lost before impacting the forced expiratory volume 1(FEV1) or FEV1/FVC ratio. Furthermore, small airway obstruction may have less effect on lung mechanics than on ventilation distribution.55, 56
Prevalence, Clinical Presentation, and Diagnosis
Recent prevalence estimates suggest that BOS is often underdiagnosed and that 14% of all long-term survivors with cGVHD may develop BOS. BOS is difficult to diagnose, may already be severe by the time the patient complains of symptoms, and is not easy to reverse.
Clinically, patients present with dyspnea on exertion, decreased exercise tolerance, or nonproductive cough, with their degree of symptomatology paralleling their degree of obstruction on pulmonary function testing (PFT). BOS usually occurs within the first 2 years, but may develop as late as 5 years after allo-HCT. Reliance upon symptoms for diagnosis can be dangerous, because once symptoms are apparent the extent of airflow obstruction may not only be significant (FEV1 < 40% predicted), but the process may be irreversible. With routine screening spirometry, BOS is often diagnosed on the basis of new airflow obstruction even before the patient is symptomatic.
BOS is diagnosed by demonstration of a fixed airflow obstruction that is defined as: (1) decreased 1-second FEV1 <75% of predicted, and evidence of airway obstruction as demonstrated by FEV1/forced vital capacity ratio of <0.7 on PFT; (2) signs of air trapping by PFT as shown by residual volume >120% of predicted, or evidence of air trapping on computed tomography or lung biopsy; (3) absence of acute respiratory infection; and (4) another manifestation of cGVHD in an additional organ system if no histologic evidence of BOS can be demonstrated.52, 55
Early identification strategies, borrowed from the field of lung transplantation, utilize serial testing of the extent of FEV1 decline from pretransplantation baseline. Early onset of BOS can have worse outcomes than late-onset BOS, suggesting that these are two distinct clinical entities that may warrant different treatment approaches.52, 55 There is growing awareness that patients with BOS have high mortality rates regardless of therapy, suggesting the need for early identification, preemptive treatment, and novel approaches.57
Prophylaxis of Chronic Graft-versus-host-disease and Bronchiolitis Obliterans Syndrome
cGVHD can be a significant complication of HCT impacting up to 80% of patients receiving alternative donor grafts. cGVHD is independently associated with late pulmonary complications and BOS is strongly associated with cGVHD.11, 57 It has been reported that the administration of antithymocyte globulin (ATG) during the conditioning regimen or early after transplant, in addition to the conventional GVHD prophylaxis, can reduce the incidence and the severity of subsequent cGVHD.56, 58 The magnitude of reduction is ˜ 20% or greater for both aGVHD grade II-IV and cGVHD.51 In comparison to those who did not receive ATG, the incidence of cGVHD was reduced from 60% to 37% (P = 0.05), and extensive cGVHD reduced from 41% to 15% (P = 0.01). Significantly, the cumulative incidence of chronic lung dysfunction was reduced from 51% to 19% (P = 0.005). Further incentive for using ATG has been found in the conclusions of prospective randomized trials with ATG, which suggest that prevention of cGVHD is possible without significantly interfering with the graft-versus-malignancy effect and may result in wider use of ATG.
Management of Bronchiolitis Obliterans Syndrome
Systemic Glucocorticoids
The mainstay of therapy has been systemic IST including high-dose corticosteroids, CSA, azathioprine, and ATG with the intent of general control of cGVHD. Sullivan et al.59 first described in 1981 use of prednisone along with azathioprine in a series of 52 patients with cGVHD as effective therapy. Since then, systemic high-dose corticosteroids have been thought to be the most efficacious treatment in cGVHD. Ratjen et al.60 showed improvement in FEV1 with 7 of 9 patients in the pediatric population after HCT with clinical stability following treatment with high-dose methylprednisolone for BOS. Despite the unfavorable side-effect profile and the absence of strong evidence, systemic glucocorticoids remain the recommended first-line therapy (dosage varies from 0.1 to 1 mg/kg/day—depending on severity) for patients diagnosed with BOS (Table 106.2).
Inhaled Corticosteroids
Inhaled corticosteroids may optimize local delivery while abrogating the risks of systemic corticosteroids in the treatment of BOS. Bashoura et al.61 used fluticasone-propionate in patients with BOS after HCT and reported stabilization or improvement in FEV1 after 3 to 6 months of treatment in 16 of 17 patients. Similarly, Bergeron et al.62 reported improvement in symptoms as well as in FEV1 at 3 to 6 months posttherapy using a combination of budesonide and formoterol. This strategy has yet to be evaluated in a prospective randomized controlled manner, but the potential to deliver high doses of steroid therapy in the inhaled modality is a promising method of improving treatment without the systemic risks.
TABLE 106.2 AVAILABLE THERAPEUTIC OPTIONS FOR BOS AFTER ALLOGENEIC HEMATOPOIETIC CELL TRANSPLANTATION (HCT)
Agent
Mechanism of Action
Systemic corticosteroids
Systemic immunosuppression
Inhaled corticosteroids
Localized antiinflammatory
Calcineurin inhibitors
Systemic immunosuppression
Mycophenolate mofetil
Inhibits fibroblast proliferation
mTOR inhibitors (e.g., sirolimus)
Inhibits fibroblast proliferation
Azithromycin
Macrolide antibiotic
Impairs neutrophilic inflammation
? prokinetic GI properties leading to reduction of GERD
Montelukast
Leukotriene receptor antagonist Reduces bronchoconstriction, eosinophilic and neutrophilic recruitment
Extracorporeal photopheresis
Mechanism not understood Involvement of regulatory T cells
Imatinib
Antifibrinogenic
Rituximab
Inhibits B cell proliferation (Anti-CD20 antibody)
Other immunosuppressive agents such as calcineurin inhibitors (cyclosporine and tacrolimus), mammalian target of rapamycin inhibitors (sirolimus and everolimus), as well as mycophenolate mofetil have also been shown to be efficacious in treatment of BOS in patients who undergo lung transplant.55
Azithromycin
Azithromycin, a macrolide antibiotic, has been shown to modulate cytokine production and impair neutrophil function. Several small studies in the lung transplant literature have shown that chronic therapy with azithromycin can improve FEV1 or slow progression of BOS.63, 64, 65 The largest study reported to date has been by Vos et al.,66 whose cohort of 107 lung transplant recipients with BOS were evaluated on long-term azithromycin therapy. Forty percent of patients were responsive to treatment, and these patients were reported to have improved OS compared with those who did not respond to macrolide therapy. The same authors have also published data that prophylactic azithromycin thrice weekly for 2 years after transplantation may prevent BOS by improving FEV1 as well as BOS-free survival in the same cohort.67 Khalid et al.68 reported significant clinical improvement in FEV1 and forced vital capacity in 7 of 8 patients with BOS after allo-HCT using azithromycin 500 mg daily for 3 days followed by 250 mg three times weekly for a minimum of 12 weeks.
Given its ease of administration and favorable side-effect profile, it is being increasingly used as upfront therapy for BOS and is recommended as adjunctive therapy in addition to corticosteroids and additional IST.
Novel Combination Therapy
Norman et al.69 have reported a small case series (n = 8) of BOS after HCT using combination therapy with fluticasone, azithromycin, and montelukast (FAM). Their results suggest that combination therapy may spare some patients from systemic steroids and is being investigated in a prospective phase II trial. A list of other therapeutic agents available in clinical practice is summarized in Table 106.2.
Lung Transplantation
Although data is limited, lung transplantation upon failure of medical therapy is also an option, with several cases reported in the literature after HCT for patients who are thought to have achieved a cure for their hematologic malignancy but have severe BOS.70, 71, 72 Currently, there are no defined criteria for the appropriate timing for referral to a lung transplant, but those who have remained in remission for years without significant comorbidities or other long-term complications from HCT may be good candidates for consideration.
INFECTION AND IMMUNE RECONSTITUTION
Infection remains an immense challenge in long-term survivors, especially in patients requiring prolonged IST for cGVHD. Infection in survivors, even in the absence of cGVHD, is over 20 times greater than reported in the general population. About 20% of patients remain on IST beyond 3 years post-HCT, with a higher incidence in older patients receiving HCT.8, 11 There is an elevated risk of bacterial, fungal, and viral infections occurring even years after HCT, although this plateaus after 2 years.73 Infections remain a significant contributor to morbidity, rehospitalization and NRM in 5-year survivors.50, 74, 75, 76, 77
Immune reconstitution of the B and T cell repertoire from the donor can be insufficient, and long-term survivors still have an increased risk of infectious diseases.8, 78, 79 cGVHD and the use of systemic IST for cGVHD are the main risk factor of long-term poor immune reconstitution after HCT.80 Immune status should be monitored periodically,34 especially in those with recurrent severe infections.
Bacterial Infection
Bacterial infections such as pneumococcal infection can be lethal, especially in patients with cGVHD. Fortunately there are effective preventive options such as antibiotic prophylaxis and vaccinations.34, 76 Prolonged antibiotic prophylaxis is generally recommended for preventing infection by encapsulated organisms among patients with active cGVHD on systemic IST. Oral penicillin is generally preferred, but consideration of susceptibility patterns may warrant other options such as second-generation cephalosporins, macrolides, or fluoroquinolones. However, because of the risks of resistance, vaccinations should always be initiated if available. Several guidelines have been published34, 76, 81; our current vaccination schedule is summarized in Table 106.3.
The optimal timing of vaccination is also important34; the guidelines recommend not postponing vaccinations with nonlive vaccines in patients with ongoing active cGVHD.82 Checking antibody titers is useful in monitoring the success of vaccination in such patients. Live vaccines are generally avoided in subjects with ongoing IST. Another investigational approach to hasten the recovery of immunity is to boost donors prior to graft collection to enhance immune recovery in the eventual recipients.
TABLE 106.3 ROUTINE VACCINATIONS RECOMMENDED FOR HCT RECIPIENTS
aA uniform specific interval between doses cannot be recommended, because various intervals have been used in studies. As a general guideline, a minimum of 1 month between doses may be reasonable.
bIf immunization is started early, consider evaluating for antibody levels and if they are low, revaccinate. Following the primary series of 3 PCV doses, a dose of the 23-valent polysaccharide pneumococcal vaccine (PPSV23) to broaden the immune response might be given. For patients with chronic GVHD (cGVHD) who are likely to respond poorly to PPSV23, a fourth dose of the PCV should be considered instead of PPSV23.
cDTaP is preferred; however, if only Tdap is available (e.g., because DTaP is not licensed for adults), administer Tdap. Acellular pertussis vaccine is preferred, but the whole-cell pertussis vaccine should be used if it is the only pertussis vaccine available.
dSee text for consideration of an additional dose(s) of Tdap for older children and adults.
eSignificant improvement of recipient response to hepatitis B vaccine posttransplant can be expected only if the donor receives more than 1 hepatitis vaccine dose prior to donation.
fFor children <9 years of age, 2 doses are recommended yearly between transplant and 9 years of age.
gMeasles, mumps, and rubella vaccines are usually given together as a combination vaccine. In females with pregnancy potential, vaccination with rubella vaccine either as a single or a combination vaccine is indicated.
Late fungal infection is associated with cGVHD and systemic IST with Aspergillus spp. being the most common pathogen.76, 83, 84 There is very limited evidence to demonstrate clinical benefit of antifungals in the setting of cGVHD; however, antifungal prophylaxis especially against Aspergillus is usually recommended for patients with severe cGVHD.85 Iron overload, a frequent finding after HCT, has shown a possible association with fungal infections and this represents a potential therapeutic target.86, 87, 88, 89 Iron overload is an established risk factor for infections in patients with myelodysplastic syndromes.90 Iron chelation or phlebotomy could not only reverse transfusional overload, but might mitigate the risk of fungal infection.
Viral Infection
Viral infections, including CMV, varicella zoster virus (VZV), and influenza are responsible for late hospitalization, morbidity, and mortality in HCT survivors and are frequently associated with cGVHD.73, 77 While most CMV reactivations occur early, recent developments in transplant techniques such as preemptive CMV treatment strategies, cord blood, mismatched-related or URD HCT, and reduced-intensity conditioning have led to the emergence of late CMV reactivation and infection. CMV seropositive recipients of CMV seronegative grafts are at particular risk for prolonged reactivation.
Acyclovir prophylaxis to prevent VZV reactivation is nontoxic, effective, and routinely recommended for at least the first year after HCT.91, 92 Longer duration acyclovir prophylaxis beyond 1 year should be considered in patients with cGVHD or systemic IST. Vaccination against VZV requires administration of an attenuated virus, and early reports are promising.93, 94 However, live vaccines should be administered no earlier than 24 months after HCT; there may be differences in the safety profiles of different vaccine brands and, as yet, no VZV vaccine has been approved for HCT recipients.
There is considerable high-level evidence that annual influenza vaccination is beneficial to HCT recipients.34, 76, 81 After HCT, the first dose is often insufficient in producing satisfactory antibody titers, but a booster dose can improve the immune response.95, 96, 97, 98 However, even with two doses of vaccine the most vulnerable HCT recipients, i.e., those who have a shorter transplant-tovaccination interval and active GVHD, might fail to be protected.95 Consequently, attention must also be paid to other proven measures, such as exploiting herd immunity by vaccinating household members and avoiding symptomatic contacts.
Only gold members can continue reading. Log In or Register to continue
 The Diagnostic and Therapeutic Approach to Hematologic Problems
The Diagnostic and Therapeutic Approach to Hematologic Problems



