complicates acute stroke in 5% to 12% of patients.31 All stroke patients should be monitored for hypoxia, with a goal of maintaining O2 saturation levels of >95%.
Table 93.1 Etiology of focal cerebral ischemia | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
 |
polymorphonuclear leukocytes and confined erythrocyte-rich regions.51 It has been suggested that red cell and mixed thrombi frequently produce hyperdense middle cerebral artery (HMCA) signs sometimes observed on CT and hypointense artery signs on magnetic resonance imaging (MRI).52
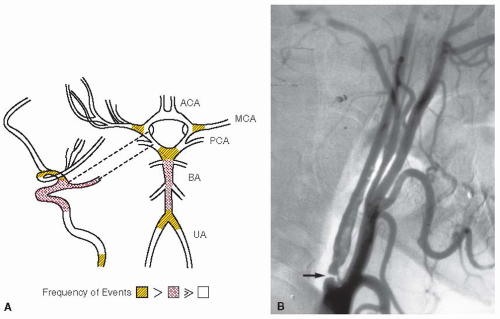 FIGURE 93.2 Atherosclerosis as a source of thrombotic and embolic obstruction of arterial circuits in the central nervous system (CNS). A: Predilection sites for atheromata in brain-supplying arteries. B: Example of severe (99%) stenosis of the ICA in patient with TIAs (arrow). ACA, anterior cerebral artery; MCA, middle cerebral artery, PCA, posterior cerebral artery; BA, basilar artery; UA, uncal artery. |
concept encompasses characteristic electrophysiologic changes, biochemical and molecular alterations, microvessel responses, metabolic changes, and regional differences in tissue perfusion and H2O diffusion as displayed by imaging studies (e.g., the DEFUSE study).93,94,95 By positron emission tomography, the infarction corresponds to rCBF below 12 mL/100 g/min and a cerebral metabolic rate for oxygen (CMRO2) below 65 µm/100 g/min.96 The penumbra has been defined as rCBF decreased to 12 to 22 mL/100 g/min, CMRO2 above 65 µm/100 g/min, and an oxygen extraction fraction of 50% to 90%.96 Experimental data from vascular and molecular modeling studies as well as recent imaging work indicate that the penumbra is dynamic and
demonstrates that in the early minutes and hours after ischemia onset the core contains pockets of injury surrounded by “minipenumbras.”93 It has been hypothesized that failure to resolve these mini-penumbras into viable tissue leads ultimately to homogenous injured tissue (FIGURE 93.5). The cell and microvessel events in large part relate to local microvascular flow and may underlie recoverability of the ischemic territory-at-risk when flow is reestablished. Normal collateral arterial circuits protect cerebral cortical tissue and may contribute to the reversibility of the ischemic penumbra. Importantly, acute reperfusion of the occluded artery (arteries) is taken to decrease the penumbra and recover normally functioning tissue.
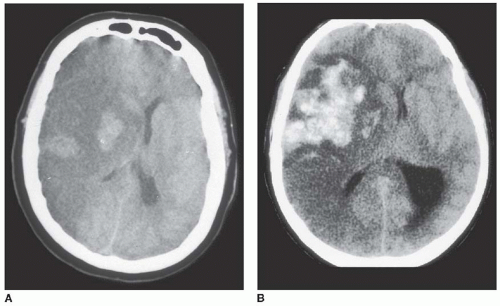 FIGURE 93.3 Hemorrhagic transformation. A: HI typified by regions of confluent petechiae 24 hours after MCA occlusion. Note midline shift due to tissue swelling. B: Parenchymal hemorrhage marked by coagulum displacing midline structures and compressing ventricle. (Image in panel A: From von Kummer R, Bozzao L, Manelf C. Early CT diagnosis of hemispheric infarction. Berlin, Germany: Springer Verlag, 1995:1, with permission.) |
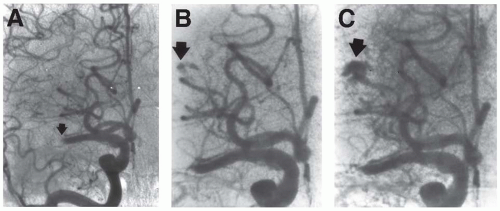 FIGURE 93.4 Evolution of parenchymal hemorrhage following intravenous infusion of recombinant tissue-type plasminogen activator (rtPA). Arrows indicate evolving hemorrhage. A: Obstruction of proximal middle cerebral artery (MCA) (M1 segment). B,C: During systemic rtPA infusion, following partial recanalization of the MCA, progressive extravasation from a distal lenticulostriatal artery was noted. A large PH with ventricular extension resulted (see FIGURE 93.3). (From the collection of M. Pessin, with permission.) |
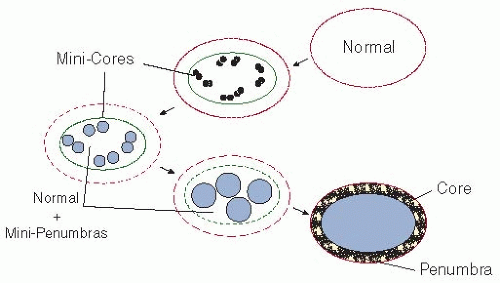 FIGURE 93.5 A proposed construct of the “penumbra” that takes into account the heterogeneous evolution of injury within the 1st hours of ischemia onset after the occlusion of a brain-supplying artery. The lesions and their reversibility depend upon the time and location of the reduction in regional cerebral blood flow (rCBF) in the territory-at-risk. If the injury stimulus cannot to be curtailed, the mini-cores coalesce with the duration of rCBF reduction devouring micro-penumbras. The evolution from normal function to the final lesion may depend upon a number of factors, including the territory of vascular supply, depth of reduction of rCBF, inflammatory state at baseline and/or degree of inflammatory response, and other factors.93 |
and specific vascular lesions (e.g., arterial dissection, small caliber vessels such as vasculitis). Imaging of the cervicocephalic vessels to demonstrate evidence and site of stenosis and occlusions is achieved by contrast-enhanced helical CT angiography.120 Image postprocessing permits the data to be visualized using multiplanar reformatting, surface or three-dimensional volume rendering, and maximum-intensity projection techniques.121 MR angiography has sensitivity and specificity ranges of 70% to 100% when compared to DSA for the detection of cervical and intracranial stenoses.122 In the intracranial vasculature, MRA is useful in identifying acute proximal largevessel occlusions, but cannot reliably identify distal or branch occlusions. Combined with data from DWI, MRA substantially improves acute diagnosis of stroke mechanism.106 Contrast-enhanced MRA techniques that employ gadolinium contrast to outline vascular structures provide more reliable images of the thoracocervical vasculature. Flow artifacts can occur, including in-plane flow saturation, susceptibility to turbulent or complex flow, and flow-like effects from adjacent short T1 substances, such as thrombus and fat, which distort the degree of stenosis.
Table 93.2 TIAs (± stroke): antiplatelet agents | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 93.3 Completed stroke: antiplatelet agents | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


