Fig. 14.1
Basal cell carcinoma gray-scale ultrasound (transverse view, tip of the nose). Hypoechoic lesion (bcc and outlined) that involves dermis and presents hyperechoic spots. The nasal cartilage is unremarkable. Abbreviations: d dermis, st subcutaneous tissue, c nasal cartilage
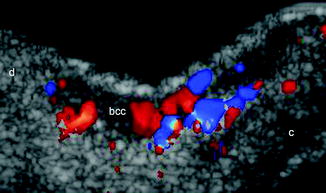
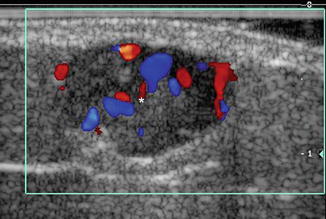
Fig. 14.2
Basal cell carcinoma color Doppler ultrasound (transverse view, tip of the nose) demonstrates increased vascularity (colors) within the lesion (bcc). Abbreviations: d dermis, c nasal cartilage
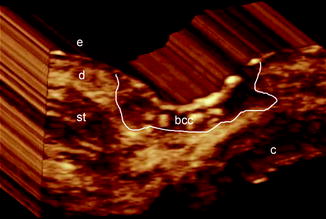
Fig. 14.3
Basal cell carcinoma 3D ultrasound reconstruction of the lesion (bcc, 5–8 s sweep, transverse view, tip of the nose). Abbreviations: e epidermis, d dermis, st subcutaneous tissue, c nasal cartilage, bcc basal cell carcinoma
Sonographic Signs in Primary Skin Cancer
Basal cell carcinoma usually appears on ultrasound as a well-defined, oval shape and hypoechoic lesion that commonly presents hyperechoic spots. Slow flow arterial and venous vessels are commonly detected at the bottom of the lesion. Occasionally, basal cell carcinoma shows pleomorphic presentations with asymmetric, bulging, lobulated or irregular appearances [12] (Figs. 14.1, 14.2 and 14.3).
Squamous cell carcinoma tends to appear as a well or ill-defined hypoechoic lesion that commonly infiltrates deeper layers (for example cartilage or muscle). Importantly, intra-lesional hyperechoic spots have not been reported in squamous cell carcinoma. Vascularity is usually more prominent compared to basal cell carcinoma. On color Doppler squamous cell carcinoma usually presents slow flow arterial and venous vessels [11] (Fig. 14.4).
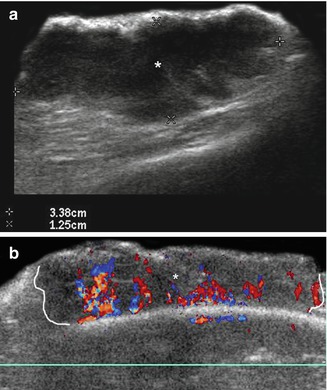
Fig. 14.4
(a, b) Squamous cell carcinoma. (a) Grey scale ultrasound (longitudinal view, left cheek) demonstrates a 3.38 cm (long) × 1.25 cm (depth) well defined hypoechoic lesion (asterisk) affecting dermis and hypodermis. (b) Color Doppler ultrasound (transverse view, frontal region) shows ill-defined hypoechoic lesion ( asterisk and outlined) that involves dermis and hypodermis. Notice the prominent blood flow within the mass (colors)
Melanoma, tend to show as a well- defined fusiform hypoechoic lesion that commonly present strong vascularity with slow flow vessels (arterial and venous). Hyperechoic spots have not been reported in melanoma. Ultrasound is also used to detect satellite (< 2 cm from the primary tumor), in–transit (≥ 2 cm from the primary tumor) or nodal metastases (Fig. 14.5). Locoregional sonographic staging of melanomas has allowed identification of the secondary involvement. The most common sonographic signs of malignant nodal infiltration are: balloon shape, nodular thickening of the cortex and loss of hyperechogenicity of the medullae. The anechoic areas frequently detected within the secondary lesions (extranodal or nodal) seem to be caused by the hypercellularity of the tumor rather than necrosis. Vascular density has been correlated with the metastatic potential in melanoma, and neovascularization has been described as a prognostic factor for metastasis equivalent to the Breslow index [3].