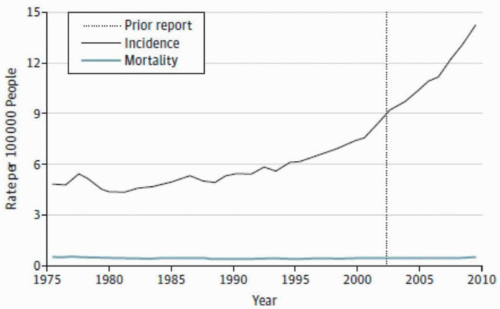
Thyroid cancer is the most common cancer of the endocrine system. It is the fifth most common cancer diagnosed in females in the United States and is increasing in incidence among both males and females, with an estimated 62,500 new cases diagnosed in 2016 (Fig. I-1).1,2,3 The primary histologic subtypes include differentiated thyroid cancer (DTC: papillary and follicular), medullary thyroid cancer, and anaplastic thyroid cancer. In recent years, both the American Thyroid Association (ATA) and the National Comprehensive Cancer Network have published guidelines on the initial evaluation of patients with thyroid nodules and thyroid cancer. These have included indications for fine-needle aspiration (FNA) biopsy, use of molecular testing for cytologically indeterminate thyroid nodules, indications for thyroidectomy and lymphadenectomy, and postoperative surveillance strategies.4,5,6,7
Given the scope of these previously published works, the intent of this section is to focus on the preoperative and intraoperative aspects of the evaluation and treatment of a patient who is undergoing surgery for a biopsy-proven papillary thyroid cancer (PTC), which is the most common subtype. In view of the low mortality rates associated with PTC, recurrence has emerged as the primary outcome of interest when determining the optimal surgical treatment algorithm in the majority of patients. Therefore, the ultimate goals of initial and reoperative surgery are to minimize rates of locoregional recurrence and to limit operative complications. Primary among these complications are permanent hypoparathyroidism and recurrent laryngeal nerve injury, which may substantially affect patients’ quality of life.8,9 Multiple studies have demonstrated that these complications occur less frequently when operations are performed by experienced surgeons and that the extent of surgery can increase the risk of complications, irrespective of a surgeon’s case volume.4,10,11,12 This work will not focus on patients with papillary thyroid microcarcinoma (cancers <1 cm), given the ongoing controversy regarding the clinical significance of the majority of these tumors.13,14,15
FIGURE I-1 New cases of thyroid cancer by histology per year in the United States (1993-2012). APC is significantly different from zero (p < 0.05). APC = annual percent change.
Clinical Staging
Using the American Joint Committee on Cancer tumor-node-metastasis (TNM) staging system (Table I-1)16 is strongly encouraged for all thyroid cancers because it provides prognostic information that can be used to guide treatment and surveillance and because it also allows for risk-stratified classification of disease that can be consistently communicated to other providers. In light of emerging data about outcomes of patients with low-risk thyroid cancer, the eighth edition of the American Joint Committee on Cancer staging system modified definitions of primary tumor and regional lymph node metastases. In addition, the age cut-off for determining disease-specific survival was changed from 45 to 55 years.16
TABLE I-1 American Joint Committee on Cancer Staging Criteria for Thyroid Cancer, 8th Edition
TABLE I-1A Definition of Primary Tumor (T)
Papillary, Follicular, Poorly Differentiated, Hürthle Cell, and Anaplastic Thyroid Carcinoma
Category
Criteria
TX
Primary tumor cannot be assessed
T0
No evidence of primary tumor
T1
Tumor ≤2 cm in greatest dimension limited to the thyroid
T1a
Tumor ≤1 cm in greatest dimension limited to the thyroid
T1b
Tumor >1 cm but ≤2 cm in greatest dimension limited to the thyroid
T2
Tumor >2 cm but ≤4 cm in greatest dimension limited to the thyroid
T3
Tumor >4 cm limited to the thyroid, or gross extrathyroidal extension invading only strap muscles
T3a
Tumor >4 cm limited to the thyroid
T3b
Gross extrathyroidal extension invading only strap muscles (sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles) from a tumor of any size
T4
Includes gross extrathyroidal extension beyond the strap muscles
T4a
Gross extrathyroidal extension invading subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve from a tumor of any size
T4b
Gross extrathyroidal extension invading prevertebral fascia or encasing the carotid artery or mediastinal vessels from a tumor of any size
Note: All categories may be subdivided: (s) solitary tumor and (m) multifocal tumor (the largest tumor determines the classification).
TABLE I-1B Definition of Regional Lymph Node (N)
Category
Criteria
NX
Regional lymph nodes cannot be assessed
N0
No evidence of locoregional lymph node metastasis
N0a
One or more cytologically or histologically confirmed benign lymph nodes
N0b
No radiologic or clinical evidence of locoregional lymph node metastasis
N1
Metastasis to regional nodes
N1a
Metastasis to level VI or VII (pretracheal, paratracheal, prelaryngeal/Delphian, or upper mediastinal) lymph nodes. This can be unilateral or bilateral disease.
N1b
Metastasis to unilateral, bilateral, or contralateral lateral neck lymph nodes (levels I, II, III, IV, or V) or retropharyngeal lymph nodes
TABLE I-1C Definition of Distant Metastasis (M)
Category
Criteria
M0
No distant metastasis
M1
Distant metastasis
TABLE I-1D AJCC Prognostic Stage Groups-Differentiated Thyroid Cancer
When age at diagnosis is…
And T is…
And N is…
And M is…
Then the stage group is…
<55 years
Any T
Any N
M0
I
<55 years
Any T
Any N
M1
II
≥55 years
T1
N0/NX
M0
I
≥55 years
T1
N1
M0
II
≥55 years
T2
N0/NX
M0
I
≥55 years
T2
N1
M0
II
≥55 years
T3a/T3b
Any N
M0
II
≥55 years
T4a
Any N
M0
III
≥55 years
T4b
Any N
M0
IVA
≥55 years
Any T
Any N
M1
IVB
Note: American Joint Committee on Cancer staging and TNM classification for differentiated thyroid cancer.16 Used with permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original and primary source for this information is the AJCC Cancer Staging Manual, Eighth Edition (2017) published by Springer International Publishing.
Only gold members can continue reading. Log In or Register to continue