(i.e., cyclosporine or tacrolimus) or methotrexate for prevention of GVHD improved survival after allogeneic marrow grafting.7, 8 It was then established that methotrexate and cyclosporine in combination were more effective than either used alone.9 The efficacy of a calcineurin inhibitor and methotrexate combined for GVHD prevention was subsequently confirmed in clinical trials and remains the standard in many transplant programs.
TABLE 102.1 DISORDERS TREATED BY TRANSPLANTATION | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
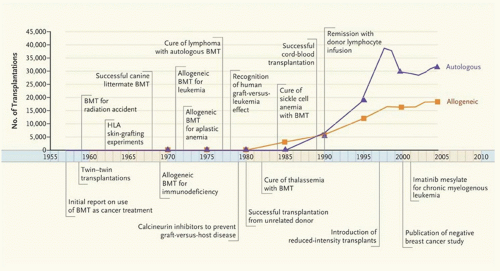 FIGURE 102.1. Timeline showing numbers of bone marrow transplantations and advances in the field, 1957-2006. BMT denotes bone marrow transplantation; HLA, human leukocyte antigen. Data are from the Center for International Blood and Marrow Transplant Research. (Reprinted with permission from Appelbaum FR. Transplantation of bone marrow as compared with peripheral blood cells from HLA-identical relatives in patients with hematologic cancers. N Engl J Med 2007;357:1472-1475. Copyright 2007 Massachusetts Medical Society. All rights reserved.) |
experimental observations may have resulted from cell fusion, technical artifact, or culture induced changes in cellular gene expression. Nevertheless, there is agreement that if “plasticity” of circulating HSCs occurs, it is likely to be a rare event.28
TABLE 102.2 CHARACTERISTICS OF HUMAN HEMATOPOIETIC STEM CELL (HSC) | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
TABLE 102.3 POTENTIAL SOURCES OF HEMATOPOIETIC STEM CELL (HSC) FOR HEMATOPOIETIC CELL TRANSPLANTATION | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
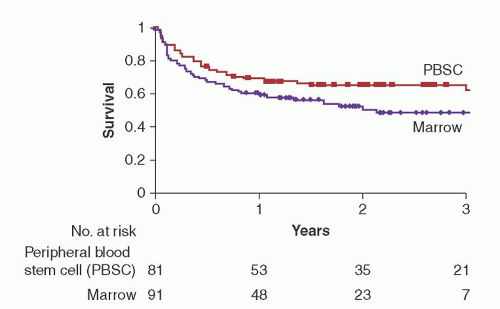 FIGURE 102.2. Probability of overall survival after myeloablative conditioning and transplantation with either peripheral blood stem cells or marrow. Survival at 2 years was improved in the peripheral blood stem cell group as compared to marrow (66% vs. 54%; P = 0.006). Disease-free survival was also improved in the peripheral blood stem cell group (P = 0.003). (Reprinted with permission from Bensinger WI, Martin PJ, Storer B, et al. Transplantation of bone marrow as compared with peripheral blood cells from HLA-identical relatives in patients with hematologic cancers. N Engl J Med 2001;344:175-181. Copyright 2001 Massachusetts Medical Society. All rights reserved.) |
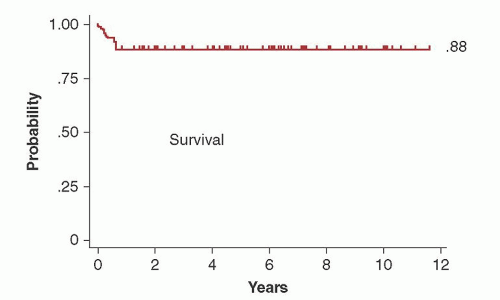 FIGURE 102.3. Overall survival among 94 patients with aplastic anemia who underwent transplantation from HLA-identical siblings after conditioning with cyclophosphamide (CY) and antithymocyte globulin. With a median follow-up of 6.0 (0.5 to 11.6) years, the Kaplan-Meier estimate of survival was 88%. Cyclosporine and methotrexate were administered after transplantation for graft-versus-host disease (GVHD) prophylaxis. (Reprinted with permission from Storb R, Blume KG, O’Donnell MR, et al. Cyclophosphamide and antithymocyte globulin to condition patients with aplastic anemia for allogeneic marrow transplantations: the experience in four centers. Biol Blood Marrow Transplant 2001;7:39-44.) |
of Epstein-Barr virus (EBV) or cytomegalovirus (CMV) is negligible compared to conventional allogeneic transplantation. HLA allele mismatches (up to 2 to 3 loci) are permissible in cord blood transplantation. Notable disadvantages to cord blood transplantation are the potential for prolonged pancytopenia and lower rates of overall engraftment.
numbers. The number of aphereses may be reduced to one or two sessions when HSC are mobilized to the peripheral blood after the administration of cytokines alone or in combination with chemotherapy or plerixafor. An effective mobilization strategy of autologous HSC for patients with malignancy is chemotherapy in conjunction with G-CSF, 6 µg/kg/day.61 After chemotherapy, patients are apheresed when the total white blood cell count has recovered to 1,000/µl or the CD34-positive cell count in the peripheral blood is at least >10/µl. For patients not requiring chemotherapy or normal allogeneic donors, mobilization is with G-CSF alone (5 to 16 µg/kg) by daily subcutaneous injections for 5 to 8 days.48, 127, 128 These doses of G-CSF are generally well tolerated, with common side effects of bone pains, myalgias, and flu-like symptoms that are managed with acetaminophen or low-dose narcotics. Plerixafor in combination with G-CSF was effective for increasing the yields of circulating CD34+ progenitor cells and is indicated for patients with lymphoma or multiple myeloma who are being collected for autologous HCT.56 The recommended dose is 0.24 mg/kg/day administered subcutaneously 11 hours before the apheresis procedure. The maximum dose is 40 mg/day. Common side effects included diarrhea, nausea, fatigue, headaches, and arthralgias. Apheresis was performed as early as day 4 after the start of G-CSF using a continuous blood flow separation technique. Apheresed products may be cryopreserved in 5% dimethylsulfoxide (DMSO) for use after thawing on the day of transplant. A more rapid sustained hematopoietic recovery of both neutrophil and platelet counts occurs with increasing numbers of CD34+ cells in the hematopoietic cell graft (up to 5 × 106/kg). Some investigators consider 2.5 × 106/kg of recipient weight a minimum dose of CD34+ cells from the peripheral blood to achieve complete autologous recovery. Platelet recovery is more rapid at higher CD34+ cell doses.60, 61 Since the cell dose used in the autologous transplant setting yields consistent and prompt engraftment, it is also considered an appropriate target for collection of allogeneic HSC from the peripheral blood. Donors of peripheral blood avoid general anesthesia and other complications of marrow harvesting. If peripheral veins are inadequate, a large bore double lumen catheter for vascular access may be required. In a large analysis of safety from the NMDP (n = 2,408 donors), it was concluded that collection of peripheral blood stem cells was safe but that nearly all patients will experience bone pain and 1 in 4 will have headache, nausea, or citrate toxicity.129 Serious and unexpected toxicities were experienced by 0.6% of the donors, but complete recovery was universal.
(1,200 cGy versus 1,575 cGy).149, 150 The relapse rate was reduced in the group of patients receiving the higher dose of TBI, but was associated with an increase in complications from regimen-related toxicity and GVHD which negated any improvement in disease-free survival compared to the group receiving the lower dose of TBI. In a more recent study, conditioning with TBI 800 cGy and fludarabine was compared with TBI 1,200 cGy and CY and there was no difference in overall survival, relapse, or treatment-related mortality.151 The combination of BU/CY was determined to be an acceptable alternative to CY/TBI for patients with leukemia in several studies.152, 153, 154 However in one study, patients in the BU/CY group had an increased risk of sinusoidal obstruction syndrome (SOS) of the liver and other transplant-related complications.155 Since this last study, it has been demonstrated that targeting of busulfan levels in the plasma may decrease the risk of relapse and severe regimen-related toxicities, contributing to an improved disease-free survival (Fig. 102.4).156 Monitoring levels of metabolites from cyclophosphamide may also be important to decrease the risk of liver toxicity and nonrelapse mortality.157, 158
Related posts:
 The Diagnostic and Therapeutic Approach to Hematologic Problems
Diagnosis and Classification of the Acute Leukemias and Myelodysplastic Syndromes
Pathology of the Myeloproliferative Neoplasms
Non-Hodgkin Lymphoma in Children
Monoclonal Gammopathies of Undetermined Significance and Smoldering Multiple Myeloma
Late Effects After Transplantation
The Diagnostic and Therapeutic Approach to Hematologic Problems
Diagnosis and Classification of the Acute Leukemias and Myelodysplastic Syndromes
Pathology of the Myeloproliferative Neoplasms
Non-Hodgkin Lymphoma in Children
Monoclonal Gammopathies of Undetermined Significance and Smoldering Multiple Myeloma
Late Effects After Transplantation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


