Gonadal Complications and Teratogenicity of Cancer Therapy
Gonadal Complications and Teratogenicity of Cancer Therapy
Catherine E. Klein
Sonia Okuyama
In recent years, the remarkable screening, diagnostic, and therapeutic advances in the practice of oncology have totally altered the prognosis for many cancer patients, adding years to their anticipated survival. Patients with high-grade lymphomas, Hodgkin disease, testis tumors, early stage breast cancer, and pediatric sarcomas are regularly cured of their malignancy; and many others will experience prolonged survival in the face of incurable but treatable disease. As patients with these once-fatal malignancies become long-term survivors, many must face the potentially devastating complications of the very therapy that has prolonged their lives. Young patients cured of these diseases must confront not only the temporary, but also the permanent, alterations in gonadal function that are now recognized as among the most prevalent long-term side effects of cancer therapy. Therefore, many young women experience symptoms of premature gonadal failure, including menopause, sterility, and presumably the accelerated osteoporosis and coronary atherosclerosis associated with estrogen deprivation (Fig. 26.1). Male survivors of cancer are routinely oligoazoospermic and infertile. The subtle decline in testosterone levels in otherwise normal aging men has been termed andropause and may be associated with mood changes, loss of libido and erectile function, bone loss, and potentially coronary and cerebral artery disease.1 It is anticipated that longer follow-up of male cancer survivors may document an increase in these complications as well. Those patients who retain fertility are faced with real concerns regarding the risk of complicated pregnancies, and birth defects, as well as the intellectual development and the future cancer risk in their offspring, should they choose to conceive.
Although many questions remain, recognition of these complications has led to better documentation of their frequency, specific risk factors, more effective counseling both pre- and post-therapy; and new strategies to ameliorate or prevent some of the toxicities through hormonal manipulation, selection of alternative treatments, or pretreatment cryopreservation of germ cells. Obviously, the detrimental effect of cancer therapy on the fertility of surviving patients is not limited to the side effects of chemotherapy. The tumor itself may impinge on the gonads. Surgery may remove or significantly impair the function of reproductive structures, as is typical for young men with testicular cancer who undergo retroperitoneal lymph node dissection or men whose prostate cancer is treated with orchiectomy. In addition, radiation therapy has long been recognized as a sterilizing and mutagenic force. Finally, the psychosocial aspects of cancer diagnosis, treatment, and recovery often leave behind profound alterations in libido and sexuality, poorly understood issues that deserve more attention.
HYPOTHALAMIC-PITUITARY-GONADAL AXIS
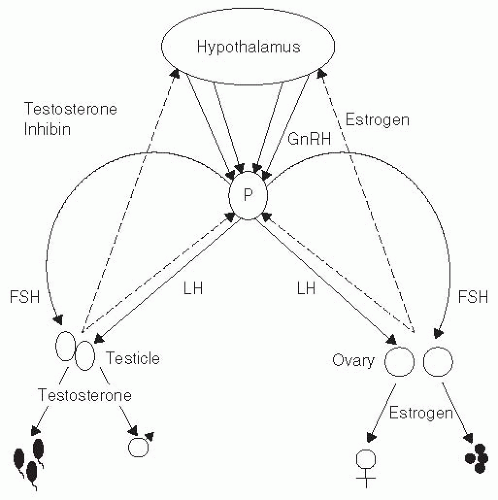
Primary regulation of both the germ cell and the endocrine function of the gonadal axis rests at the level of the hypothalamus (Fig. 26.1), where neurosecretory cells synthesize and release in a pulsatile fashion gonadotropin-releasing hormone (GnRH) into the hypothalamohypophysial-portal circulation. In response to GnRH, gonadotrophs in the anterior pituitary synthesize and release the gonadotropins follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which ultimately control gonadal function. In women, FSH stimulates ovarian follicles to grow and mature, whereas LH stimulates ovulation and corpus luteum formation. This is seen clinically as normal menstrual cycling and appropriate levels of LH, FSH, estrogen, and progesterone. In normal men, FSH initiates, and testosterone sustains, spermatogenesis. LH controls androgen synthesis by the testicular Leydig cells.2 In both men and women, primary gonadal failure results in increased LH levels, from loss of the negative feedback of estrogen at the hypothalamus and pituitary in women, and decreases in both androgen and estrogen feedback in men.3 In response to decreased levels of sex steroids as well as the loss of inhibin, FSH levels are also elevated after gonadal damage. In women, a period of partial functioning may precede frank ovarian failure. This interval is characterized by sporadic, irregular menstrual cycling, with generally diminished estrogen and progesterone levels and correspondingly elevated gonadotropins. Women may conceive, however, during the normal ovulatory cycles. In men, spermatogenesis declines, but in the absence of extreme gonadal compromise, endocrine function is generally preserved, albeit at the expense of elevated LH and FSH levels. In both sexes, germinal function may not be damaged in parallel with endocrine function, so that FSH and LH elevations may be somewhat asynchronous. Nevertheless, the hallmark of primary gonadal failure from any cause is some pattern of elevation of gonadotropin levels, and this is the usual state in postpubertal patients receiving substantial doses of antineoplastic agents.
Historical Background
The effects of radiation and cytotoxic agents on gonadal functions have been recognized for most of the last century. The radiosensitivity of the testes was noted in animals as early as 1903 and was repeatedly confirmed over the next 50 years.4,5 Atomic Energy Commission studies of normal men, completed in the 1960s, documented the extraordinary sensitivity of spermatogonia to as little as 10 cGy of irradiation, a dose approximately one-third that required in mice to produce equivalent damage.6 After a single dose of 500 cGy to the testicle, 50% of men are rendered permanently sterile. Oocytes, although more resistant, nevertheless demonstrate a dose-dependent sensitivity to irradiation, and at reproducible radiation doses, women also experience permanent sterility and premature menopause at a frequency that increases with age. As with testicular radiation, a single dose of 500 cGy to the ovaries is associated with predictable amenorrhea that persists for up to 18 months, and essentially all women >40 are rendered permanently infertile.7 Secondary infertility has been reported in association with radiation administered to the hypothalamus or pituitary in conjunction with therapy for intracranial neoplasms.8 It is important to bear in mind the extreme sensitivity of the human gonad to the sterilizing effects of radiotherapy, as many of the studies from which the risk of infertility from cancer therapy is derived are confounded by the coadministration of X-ray therapy with the drugs discussed below.
Figure 26.1 The hypothalamic-pituitary-gonadal axis and secondary sexual development. The secretion of GnRH from cells in the hypothalamus controls the pulsatile release of LH and FSH from the pituitary gland (P). These in turn regulate gamete production and sex steroid biosynthesis at the gonadal level. Feedback of sex steroids occurs at both the pituitary and hypothalamic levels.
Initial reports describing the detrimental effects of chemotherapy on human male reproductive function appeared shortly after the radiation toxicity was recognized,9 but by the 1940s, case reports had been confirmed by a pathologic study of the testes obtained from 30 men who received nitrogen mustard. Twenty-seven of these men had significant testicular atrophy and absent spermatogenesis.10 In women, the first convincing documentation of menstrual irregularities or amenorrhea following the administration of cancer chemotherapy appeared in 1956, when Louis et al.11 reported a small series of four young women being treated with busulfan for chronic myelogenous leukemia, all of whom developed menopausal symptoms within 3 months of starting therapy. Ovarian histology and endometrial histology were consistent with primary ovarian failure.
Shortly thereafter, it was recognized that other alkylating agents, including nitrogen mustard, chlorambucil, and cyclophosphamide, when given in sufficient doses, produced the same effects.12,13,14 A number of other chemotherapeutic agents of varying classes have subsequently been added to the list of presumed or possible ovarian toxins (Table 26-1).
Many other commonly used drugs, however, have poorly documented effects on gonadal function in either men or women, and much of what is known has been inferred from published series documenting frequent ovarian failure or impaired spermatogenesis in association with combination chemotherapy for diseases with extended survival: Hodgkin disease, breast cancer, and acute lymphocytic leukemia.15,16,17,18,19,20 Therefore, the sensitivity of dividing germ cells to chemotherapeutic agents or to radiotherapy has been recognized from the very onset of their use, but until recently, the frequency and severity of toxicity were considered somewhat irrelevant and were poorly appreciated.
Preclinical Studies
Although the effects of chemotherapy and radiotherapy on gonadal function have been extensively documented in humans, a number of preclinical models have been useful in better defining the nature and the mechanism of germ cell damage and in developing potential methods for circumventing these problems. Most animal studies have evaluated alkylating agents in male rodents and have found that these drugs uniformly produce marked inhibition of DNA synthesis in the differentiating spermatogonia while relatively sparing the slowly dividing stem spermatogonia population.21,22,23 Similar findings, largely limited to the alkylating agents, have been reported in dogs and monkeys.24,25 Within the post-stem cell spermatogonial population, however, there appears to be a distinct species-specific and drug-specific variation in susceptibility. Whether this differential sensitivity with the stage of spermatogenesis is also characteristic of human males has been difficult to establish.
In most animal systems, male infertility is reversible. In contrast to other alkylating drugs, however, chronic procarbazine administration can produce permanent sterility in male rodents.21 The very high frequency of long-term infertility seen in survivors of Hodgkin disease treated with nitrogen mustard, mechlorethamine, Oncovin (vincristine), prednisone, procarbazine (MOPP) or other procarbazine-containing combinations suggests that procarbazine may be significantly more toxic than other alkylating drugs in humans as well. In a cross-sectional study on the effects of doxorubicin (Adriamycin), cytosine arabinoside, bleomycin, cyclophosphamide, hydroxyurea, vinblastine, and vincristine given as single injections to male mice, doxorubicin appeared to be the most toxic to stem cells.26 Gemcitabine seems to impair spermatogenesis acutely in a mouse model.27 Presumably because of their relative specificity for the S phase of the cell cycle, the antimetabolites, even when used in high doses, have not been associated with long-term gonadal damage. Other newer agents are also being reported. For example, arsenic trioxide in male mice impaired sperm mobility and viability via reduction of gene expression of certain key enzymes involved in testosterone synthesis.28
Table 26-1 Relative Risks of Diminished Germ Cell Function Associated with Common Chemotherapeutic Agents
Frequency
Males
Females
Common
Cyclophosphamide
Cyclophosphamide
Nitrogen mustard
Nitrogen mustard
Procarbazine
Procarbazine
Nitrosoureas
Nitrosoureas
Chlorambucil
Busulfan
Melphalan
Thalidomide
Possible
Vinblastine
Vinblastine
Carboplatin
Carboplatin
Cisplatin
Cisplatin
Cytosine arabinoside
Cytosine arabinoside
Etoposide
Etoposide
Ifosfamide
Actinomycin D
Corticosteroids
Hydroxyurea
Taxanes
Taxanes
Thioguanine
Tamoxifen
Chlorambucil
Rare
Vincristine
Vincristine
Doxorubicin
Doxorubicin
MTX
MTX
5-Fluorouracil
5-Fluorouracil
Imatinib
Imatinib
Navelbine
Navelbine
6-Mercaptopurine
Dacarbazine
Bleomycin
Bleomycin
Interferon
Interferon
Azathioprine
No data
Gemcitabine
Gemcitabine
Oxaliplatin
Oxaliplatin
Irinotecan
Irinotecan
Pemetrexed
Pemetrexed
Bendamustine
Bendamustine
Azacytidine
Azacytidine
Targeted antibodies
Targeted antibodies
Interleukin
Ifosfamide
More recently, quite interesting findings have been reported by the Canadian group led by Robaire et al., who have studied the reversibility of gonadotoxic effects on male rats from commonly used combination chemotherapeutic regimens. The bleomycin, etoposide, and cisplatin (BEP) regimen for testicular cancer caused reduced testicular weight and impaired spermatogenesis with germ cell apoptosis. These exposed rats were still able to impregnate the (untreated) female rats, although litter size was decreased because of preimplantation and postimplantation losses. Only preimplantation losses persisted while the rest was reversible.29 The CHOP regimen for non-Hodgkin lymphoma caused similar issues, noting increased spermatozoal DNA damage as well. Initially impaired progeny outcomes were reversed with time, but germ cell DNA breaks remained elevated.30
Few animal studies evaluating ovarian function have been published, as there are very limited animal models for drug-induced female infertility.31 In female rats, alkylating agents appear to selectively target the medium and large follicles. Once the animal has become hypogonadal, the compensatory pituitary increases in gonadotropins may recruit the relatively resistant small follicles into the more sensitive pool, thereby aggravating the damage.32 Newer xenografting animal models are promising. In one such model, subcutaneously engrafted human ovarian tissue into immunodeficient mice was validated as a useful model with the use of cyclophosphamide.33
Chemotherapy Effects in Boys
In contrast to the profound gonadal damage with subsequent elevation of gonadotropins and diminished spermatogenesis in adult men receiving nitrogen mustard therapy, reports of chemotherapy administered to prepubertal and pubertal boys suggested that the less mature testicle might be relatively resistant to drug-induced effects. This assumption was predicated on the finding of relatively normal LH and FSH levels in these young patients posttherapy. However, since those earliest reports, a number of histologic studies have been published, all of which demonstrated significant structural damage to the testicle, even in young boys.
Although levels of LH, FSH, and serum testosterone after chemotherapy in prepubertal boys may be normal, testicular biopsies from boys receiving combination therapy for acute lymphoblastic leukemia or Hodgkin disease commonly show seminiferous tubular damage and interstitial fibrosis.34,35 Consistent with their normal hormone panels, the vast majority of boys progress normally through puberty after chemotherapy, only rarely needing androgen supplementation. Even when testicular biopsy shows that <50% of seminiferous tubules contain identifiable spermatogonia, >90% of prepubertal or pubertal boys demonstrate normal basal and stimulated hormone panels.36
Perhaps a better reflection of the major disruption of seminiferous tubular histology, however, is the relatively high incidence of significant reproductive dysfunction as measured by subsequent assessment of sperm count, morphology, and motility. Although the exact frequencies reported vary widely,36,37,38 it is clear that the immature male gonad is at major risk for permanent damage affecting the ultimate fertility of the patient. The frequency of normal sperm counts in a series of pubertal or prepubertal patients treated with single-agent cyclophosphamide, for example, even years after therapy, has been reported to range between 0% and 100%.38,39,40 A review of oral cyclophosphamide administered in cumulative doses of 0.7 to 52.0 g revealed gonadal damage in 10 of 63 (16%) prepubertal boys, whereas 10 of 15 (67%) pubertal boys had evidence of gonadal dysfunction.41
Other drugs have been associated with similar long-term disruption of gonadal function. Chlorambucil, given alone or in combination with prednisone and azathioprine for the treatment of renal disease in patients ranging from 6 to 15 years of age produced azoospermia in 17 of 21 patients, persisting 3 to 11 years after cessation of treatment.42 Nitrosoureas used for childhood brain tumors have been associated with testicular failure.43 As Leydig cell dysfunction is only rarely documented, prepubertal damage to spermatogenesis can be assessed only with testicular biopsy or long-term follow up of fertility, and it is possible that much of the difference in testicular susceptibility to chemotherapeutic agents previously attributed to pubertal stage may actually represent inappropriate assessment.
The cumulative dose of the drug administered appears to be the other major factor important in determining the degree of injury to testicular function associated with cytotoxic chemotherapy use in prepubertal boys. This dose-response relationship is especially clear for the alkylating agents. A large meta-analysis of 30 studies comprising 456 patients treated with cyclophosphamide (either alone or in combination with other cytotoxic agents or prednisone) for renal disease, Hodgkin disease, or leukemia, with no confounding exposure to either abdominal or gonadal radiation, found that the cumulative dose of cyclophosphamide had a profound effect on subsequent spermatogenesis assessed after reaching sexual maturity. Although <10% of prepubertal boys who received <400 mg per kg cyclophosphamide total dose demonstrated gonadal dysfunction, the incidence rose to 30% in those who received 400 to 500 mg per kg or >500 mg per kg.44 Of note, the pubertal stage again exerted an independent, significant influence on the incidence of dysfunction, which varied between 0% and 24% in prepubertal boys and climbed to 68% to 95% in sexually mature adults. In many small series, a confounding effect of nutritional status can be shown to play an important role in determining the recovery of the spermatogenic epithelium in prepubertal boys who receive chemotherapy. Nevertheless, drug-dose and maturational stage of the testicle appear to be the major determinants of the degree of damage to spermatogenesis in chemotherapy patients. Hormonal function remains relatively intact.45
MOPP chemotherapy given to boys frequently produces significant impairment in subsequent spermatogenesis, and infertility has been reported to last for years.38,46 Remission induction for childhood acute leukemia, with combinations including methotrexate (MTX), cytosine arabinoside, and vincristine, seems to exert a less permanent impact on spermatogenesis in boys.36 Prednisone, when used in adults, is associated with reversible oligospermia, but no information is available for children. Unfortunately, there are many poorly understood exceptions to these general trends, and reliable predictions for any given patient are impossible. Assumptions cannot be made that even minimal doses of chemotherapy given to prepubertal children will not result in permanent sterility, and short of testicular biopsy, there remains no good measure of gonadal damage until seminal analyses at puberty can be assessed.46
As described in single-agent therapy, Leydig cell function in prepubertal males seems to be somewhat more resistant to multiagent chemotherapy than does the germinal epithelial function. Gynecomastia associated with elevated FSH and LH levels was reported in 9 of 13 pubertal boys receiving MOPP treatment.47 However, among four prepubertal boys who received the same four-drug regimen, all had normal basal and stimulated gonadotropin tests.38 Impaired spermatogenesis lasting years could be documented in most of these studies. Similarly, only 2 of 44 boys who recovered from acute lymphoblastic leukemia therapy had abnormal testosterone responses to human chorionic gonadotropin challenge, and gonadotropin secretion was normal in 29 of 32 patients studied.37 A more recent report of 40 men treated for childhood Hodgkin disease found that 26 of 28 who had received chemotherapy had elevated gonadotropin levels but normal serum testosterone and appropriate secondary sexual characteristics. However, 11 of 13 tested were azoospermic, and these changes persisted up to 17 years after treatment.48
In sum, these data indicate that the seminiferous tubules of prepubertal boys are damaged by alkylating agents or by alkylator-containing combination chemotherapy, generally in an age- and dose-dependent manner, but that the endocrine secretory pathways of prepubertal and pubertal boys function relatively normally after chemotherapy for childhood cancer. Assessment is difficult, and absolute predictions are impossible.
Chemotherapeutic Effects in Adult Men
As single agents, the alkylating drugs damage the seminiferous epithelium. The duration and extent of the injury appear to be related to the age of the patient and the amount of the drug received, much as is observed in children. Cyclophosphamide administered in total doses of 9 g results in azoospermia in all men, but this is generally reversible even with total doses as high as 18 g,49 although full recovery may take up to 3 to 4 years. Doses of chlorambucil as low as 400 mg have been associated with azoospermia in some men. Recovery may be prolonged and is probably related to total dose. Cheviakoff et al.50 reported that after a mean dose of 1,464 mg, evidence of gonadal recovery may appear approximately 40 months after cessation of therapy. As in animals, procarbazine appears to be the single most toxic chemotherapeutic agent to the adult male gonad. Although no studies of this drug as a single agent are available, inference can be drawn from multiple studies in Hodgkin disease, in which patients received combination chemotherapy, either with or without procarbazine. Nineteen of 19 patients in one study treated with cyclophosphamide, vincristine, procarbazine, and prednisone (COPP) remained oligospermic 11 years after therapy, whereas 7 of 10 treated with cyclophosphamide, vincristine, and prednisone (COP) without procarbazine had return of spermatogenesis within 3 years.19,51
MTX appears to exert minimal long-term testicular toxicity. Even when given over extended periods of time, only minor alterations in spermatogenesis can be documented, and these resolve within the first few weeks of therapy being stopped. After high-dose MTX therapy, oligospermia may be somewhat more common and protracted, with a reported incidence of 50%,52 but recovery should be anticipated within 1 to 2 years. Little information is available with which to assess the potential gonadal toxicity of either single-agent vincristine or vinblastine. The slightly lower incidence of male infertility with the MOPP combination than with mechlorethamine, vinblastine, prednisone, and procarbazine (MVPP; with vinblastine substituted for vincristine), when used for the treatment of advanced Hodgkin disease, suggests that vincristine may be slightly less toxic than vinblastine.53 Although studies of single-agent doxorubicin are also not available, it appears to have minimal long-term effect when used in combination therapy that does not include cyclophosphamide. When used with cyclophosphamide, however, it appears to augment the toxicity of that drug.54 Taxane-based chemotherapy has indirect evidence of testicular damage.55 Long-term administration of azathioprine to men with inflammatory bowel disease does not seem to affect semen quality. Long-term treatment with interferon for hepatitis C patients seems to be associated with normal gonadal hormone levels. Although very limited information is available regarding newer targeted agents, successful and normal pregnancies have been reported from men undergoing treatment with dasatinib56 and imatinib.57 No published studies are available for other targeted agents such as sorafenib, gefitinib, or bevacizumab and their potential for toxicity on male gonadal function.
An often-overlooked suppression of spermatogenesis occurs in association with corticosteroid administration. Within a month of beginning moderate-dose prednisone, profound oligospermia with marked sperm dysmotility is seen in most men. Reversibility, however, is the rule.58
With increasing numbers of long-term cancer survivors after treatment with curative combination chemotherapy, multiple reports have documented permanent infertility among patients with Hodgkin disease, non-Hodgkin lymphomas, seminomas, and the nonseminomatous testicular cancers (Table 26-2). For incompletely understood reasons, even before therapy, as many as 30% of young men presenting with Hodgkin disease are oligospermic when first evaluated, and disorders of sperm motility and morphology are probably even more common.59,60 This phenomenon appears poorly correlated with stage or extent of disease or with the age of the patient. One German series suggested that elevated erythrocyte sedimentation rate and advanced stage were the best predictors of pretreatment infertility.61 Despite frequently elevated gonadotropin levels and abnormal testicular histology, return of normal function is anticipated when treatment is completed without gonadotoxic therapy. This observation significantly confounds the interpretation of posttherapy studies. In a prospective study of 37 men receiving the MVPP combination, 12 had low sperm counts before beginning treatment, but 14 of 14 studied after 2 cycles were azoospermic. Twenty-seven of 27 remained azoospermic in the first 12 months after treatment.62 In general, after therapy for Hodgkin disease, when MOPP-like regimens (nitrogen mustard, vincristine/vinblastine, procarbazine, and prednisone) are used, evidence of diminished spermatogenesis appears early in therapy, and infertility is universal by the third cycle. After completion of treatment, the recovery rate remains very poor. Retrospective analyses of men off therapy for >2 years suggest that only 5% to 15% ever regain effective spermatogenesis.41 MOPP may be associated with slightly better recovery rates than MVPP, although there are no direct comparisons available. In contrast to the effect on spermatogenesis, Leydig cell function, although frequently impaired, seems well compensated; despite elevated gonadotropin levels and low-normal serum testosterone levels in most treated adults, few, if any, of these men require androgen replacement.46,51 Occasional men develop gynecomastia.63
Reports from a randomized prospective study comparing MOPP chemotherapy with the ABVD regimen (doxorubicin, bleomycin, vinblastine, and dacarbazine) for the treatment of advanced Hodgkin disease provide convincing evidence that the latter combination produces less gonadal toxicity in both men and women.63,64 Because it is equally efficacious in the induction of long-term remissions, ABVD should be the treatment of choice in men who are concerned about preservation of reproductive potential. Early reports of other non-MOPP regimens are also encouraging.65,66 Few studies are available with which to evaluate other combinations used more commonly in the treatment of non-Hodgkin lymphomas. Scattered small reports suggest that the COP regimen without the procarbazine may be less toxic than MOPP or COPP.51,67 A recent analysis of 14 men treated with doxorubicin, etoposide, vincristine, cyclophosphamide, and bleomycin for either Hodgkin disease or non-Hodgkin lymphoma suggests that this may be an efficacious, relatively nontoxic regimen.68
Evaluation of combination therapy for the induction of remission for acute leukemias is available largely for children and adolescents. Few series of adults have reported enough long-term survivors for adequate follow up. Nevertheless, it appears that adult survivors of leukemia may fare somewhat better than their Hodgkin disease counterparts, provided abdominal or testicular irradiation has not been used.69,70 For example, Kreuser et al.71 found that 10 of 10 patients, 14 to 38 years old, treated for acute leukemia, demonstrated recovery of spermatogenesis by the second year of maintenance therapy. From limited data available, both allogeneic and autologous bone marrow transplantation for leukemia significantly increase the risk of long-term infertility.72
Table 26-2 Gonadal Effects of Combination Chemotherapy in Males
Young men presenting with testis tumors are even more likely to demonstrate evidence of spermatogenic dysfunction at diagnosis than are young Hodgkin disease patients. In a prospective series of 41 patients, Drasga et al.73 reported that 77% were oligoazoospermic and 17% azoospermic at initial presentation, leaving only 6% with adequate sperm counts with which to undertake cryopreservation. Other studies have reported oligospermia in up to 95% of newly diagnosed patients, an incidence far higher than is seen in either Hodgkin disease or other disseminated cancers.59,74 Abnormalities of sperm motility are even more common. Pretreatment testicular histology reflects these statistics and demonstrates spermatogenic arrest, hyalinized tubules, or totally absent tubules with only viable Sertoli cells evident.75 The etiology of this phenomenon is unknown, but some relation to elevated levels of human chorionic gonadotropin or the increased local heat from the tumor has been proposed. Others have demonstrated sperm autoantibodies that are postulated to result when the blood-testis barrier is breached by invading tumor. Pretreatment FSH levels may provide a useful marker to predict the potential for posttherapy recovery of spermatogenesis.76
After 2 months of therapy with cisplatin, vinblastine, and bleomycin, with or without doxorubicin, 94% of young men in Drasga’s study were azoospermic. Patients completing therapy with either vinblastine, Adriamycin (doxorubicin), and bleomycin or cisplatin, vinblastine, and bleomycin demonstrate severe oligospermia in 75% to 100% of instances, and elevations of FSH levels are common.73,77 However, in contrast to the MOPP-treated Hodgkin patients, most studies show a timedependent recovery of spermatogenesis, with approximately 50% of patients recovering some sperm production after 2 years, and most patients within 3 years. Some evidence suggests that 400 mg per m2 of cisplatin may represent a threshold for permanent infertility. Limited data also indicate that ifosfamide may be associated with less permanent injury in this setting than what might be inferred from data with cyclophosphamide.78 A small Japanese series of 27 patients found that half of them, who had received high-dose chemotherapy including carboplatin, etoposide, and ifosfamide, were able to recover spermatogenesis and that no association with the cumulative dose of drug administered was evident.79 Disorders of sperm motility may linger considerably longer.80,81,82 Subclinical Leydig cell dysfunction, however, may have other poorly recognized sequelae. For example, a Dutch center studied long-term survivors of metastatic testicular cancer and found an incidence of coronary heart disease that was seven times higher than expected, along with a higher incidence of hypercholesterolemia and obesity, in conjunction with lower testosterone and elevated LH and FSH. They hypothesize that there is a metabolic consequence of long-term gonadal toxicity from these survivors.83
Both abdominal radiation therapy, which is associated with almost 100% azoospermia, and retroperitoneal lymph node dissection, which affects ejaculatory function, appreciably decreases the likelihood of fertility in survivors of testis tumors.77 Modifications in surgical technique in recent years have significantly decreased the incidence of retrograde ejaculation following.
Testicular function in male survivors of other tumor types has been less well studied. Shamberger et al.52 reported that three of five patients who had received adjuvant doxorubicin-based therapy for sarcoma recovered normal sperm counts, although concomitant radiation to the abdomen and pelvis or thigh and even more distant sites reduced the recovery rate substantially in 20 other patients studied. A similar study by Meistrich et al.84 estimated that 28% of men recovered satisfactory sperm counts after doxorubicin-based adjuvant treatment for osteosarcoma. Generally, testosterone levels remain adequate after cancer therapy, although occasionally elderly men with various forms of cancer develop gynecomastia, presumably as a result of a testosterone-estrogen imbalance.
Only gold members can continue reading. Log In or Register to continue