Fig. 32.1
Preoperative photographs of an ideal candidate for a Goldilocks procedure with large, highly ptotic breasts following weight loss surgery. Scars from laparoscopic bariatric surgery are highlighted
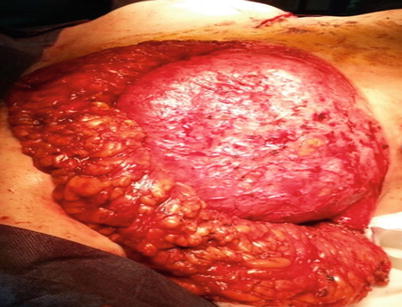
Fig. 32.2
Intraoperative photograph showing very large inferior de-epithelialised skin flap after folding to create the breast mound, prior to re-draping with the superior skin flaps and ultimately placement of the free nipple graft

Fig. 32.3
Early (2 weeks) post-operative photograph after goldilocks procedure. A Wise pattern mastectomy has been performed and the inferior skin flap de-epithelialised and folded to provide the new breast mound. The superior skin flap has been closed, and free nipple grafting has been performed

Fig. 32.4
Six months post-operative photographs
32.2 Advantages
Suitable for women not usually considered for breast reconstruction because of the combination of:
Surgical risk factors (obesity, age, comorbidities)
Larger breasts requiring a complex reconstructive plan
Relatively simple and safe one-stage autologous breast reconstruction with no donor site morbidity or implants
May tolerate postmastectomy radiotherapy (RT) (similar to a conserved breast)
32.3 Disadvantages
Limited applicability:
Not suitable for small- to moderate-sized breasts with limited ptosis
Can only be performed at the time of mastectomy
Requires meticulous surgical technique to prevent dermal flap fat necrosis and wound healing problems
Difficult to get an aesthetic outcome comparable to other autologous or implant-based techniques
32.4 History
This technique of breast reconstruction after mastectomy was first described in 1960 [1], then fully described as the Goldilocks procedure in 32 breast cancer patients (50 breasts), by Drs Heather Richardson and Grace Ma in 2012 [2]. They proposed that this relatively simple autologous (local flap) breast reconstruction technique could allow women who may otherwise not be good candidates for more conventional reconstruction techniques (usually because of age, obesity, comorbidities, etc.) to undergo a breast reconstruction. Dr. Tomoko Ogawa has described a small series of five obese Japanese women with variable aesthetic outcomes [3], and Dr. Schwartz from the USA has described a Goldilocks procedure with a free nipple graft [4].
Richardson and Ma were the first to use the term «Goldilocks» procedure. The name was inspired by a popular twentieth-century English language fairy tale character [5] who found herself in the house of Mummy, Daddy and Baby bear, she tasted porridge that was too hot and too cold then lay in beds that were too soft and too hard: finally she chose Baby bears’ porridge and bed because they were «just right». Correspondingly, the Goldilocks mastectomy represents a «just right», comprise between the extremes of breast amputation with no reconstruction or complex reconstruction.
32.5 Background
There is little published on the Goldilocks procedure, but technically it has evolved from well-established aesthetic and reconstructive techniques and there is an extensive literature base describing a variety of potential uses of de-epithelialised dermal flaps to remodel or reconstruct the breast.
32.5.1 De-epithelialised Dermal Flaps in Plastic Surgery
Reduction mammoplasty for severe breast hypertrophy (macromastia) or gigantomastia (where 1–2 kg of tissue may be removed per breast) is a technically challenging procedure. The long pedicle required to preserve the nipple areolar complex (NAC) may increase the risk of nipple necrosis so the standard approach is simple breast amputation through a Wise pattern incision with free NAC grafting onto a de-epithelised dermal bed [6]. However as with the Goldilocks procedure, this technique results in a flat wide breast with minimal projection. A number of modifications have been described to preserve sufficient dermoglandular tissue on a standard pedicle around which the skin flaps can be draped to allow a more projected breast mound [7, 8].
Kollias and colleagues [9] in Australia have described the breast amputation/inferior pedicle mound technique for reducing the contralateral breast in women with breast hypertrophy when the index breast has been removed for cancer.
32.5.2 De-epithelialised Dermal Flaps in Implant Breast Reconstruction Surgery
Following mastectomy and implant reconstruction through a Wise pattern incision, the lower pole de-epithelised dermal flap can provide implant support and coverage similar to that described for acellular dermal matrices (ADMs) and meshes [10, 11]. As the dermal flap is a living autologous tissue, it has advantages over manufactured meshes or acellular animal derived dermal matrices (ADM). The vascularised flap lies behind the vulnerable «T» junction (angle of sorrow) so protecting the implant if there is any T junction dieback [12]. For subpectoral implant reconstruction, the dermal flap can be sutured to the lower border of the elevated pectoralis major, or alternatively it may be sutured to the anterior surface of pectoralis major for prepectoral implant placement [13]. The dermal flap can also be used in combination with an ADM or meshes if required.
32.6 Indications for the Goldilocks Approach
32.6.1 Women Not Suitable for Standard Breast Reconstruction (Obese, Comorbidities, Older)
The Goldilocks approach can be considered for women who are not suitable for standard breast reconstruction techniques and would otherwise have a simple mastectomy with no reconstruction. The mastectomy can be oncologically indicated or a woman’s preference to manage her cancer, or it may be for risk reduction in high penetrance gene carriers or those with a high-risk family history.
Reconstruction may not be possible or recommended because of a range of patient factors that might restrict reconstruction choices (e.g. a large body habitus with large breasts may not be suitable for implants, and the corresponding obesity may contraindicate a DIEP) or because the risks of prolonged time on the operating table, anaesthesia and post-operative recovery is unacceptable for whatever reason.
Usually women deemed not suitable for breast reconstruction are older with multiple comorbidities such as diabetes, hypertension and smoking, often compounded by obesity (BMI > 30). Richardson and Ma commented that such women automatically exclude themselves from reconstruction as clinicians are usually focused on simplifying the treatment process to minimise risk and the need for multiple interventions and complex follow-up.
As life expectancy continues to increase in the EU [14] where the average life expectancy of a woman in Spain is now 86 years, the Goldilocks procedure may offer the opportunity of reconstruction to older women who may not wish to undergo more major autologous procedures and for whom implants are not age appropriate. Older women also tend to exclude themselves from reconstruction often because of its perceived risks and complexities [15].
32.7 Patient Selection
32.7.1 Large Ptotic Breasts
Patient selection is crucial to the success of this approach. The Goldilocks technique is essentially an extreme reduction mammoplasty: so to create enough volume to give any semblance of a breast shape, patients require ample skin and subcutaneous adiposity between the inframammary fold and nipple.
A successful Goldilocks procedure requires the combination of obesity and a large breast (macromastia) with grade 3 or 4 ptosis (Regnault’s classification [16]. The definition of macromastia is variable and not standardised, but in short there has to be sufficient lower pole skin and adiposity to give a volume that will create an aesthetically acceptable breast mound. A large breast with limited ptosis and a limited inframammary fold (IMF) to NAC distance or a very ptotic but involuted thin breast will have insufficient lower pole dermal/subcutaneous fat to create a convincing breast mound.
32.8 Contraindications
32.8.1 Previous Breast Radiotherapy
Previous breast RT may compromise the vascularity of the lower pole tissue and increase the risk of post-operative wound healing problems and fat necrosis of the dermal flap. In the Richardson and Ma paper, two women had undergone previous RT.
The poorly informed patient with high aesthetic ideals.
32.8.2 Oncology
The Goldilocks procedure is contraindicated in the following circumstances:
Whenever skin sparing mastectomy is not considered oncologically safe (e.g. inflammatory cancers).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







