Gastrointestinal (GI) side effects are very common with most chemotherapeutic and targeted agents (biologics). Most experts feel that the toxicities are generally underreported.1,2,3 It is sometimes hard to distinguish GI symptoms due to underlying malignancy from the effects of the therapeutic drug per second. This chapter discusses the therapeutic toxicities seen in the GI tract. It is very important for clinicians to be aware of the toxicities of therapeutic agents used to treat cancer and to be abreast of the latest treatment options, in order to avoid unnecessary delays/dose reductions in treatment.
The most common GI toxicities include stomatitis or oral mucositis, dysgeusia (also known as taste perversion), esophagitis, dysphagia, odynophagia, gastritis, nausea and vomiting, liver function abnormalities, enterocolitis, bowel perforation, diarrhea, and constipation. An indirect effect of GI disturbance is malnutrition. Other less common manifestations include pancreatitis, malabsorption, and infections of the GI tract (such as candidiasis, herpes virus, or CMV infection in the immunosuppressed). In this era of targeted therapy, practitioners need to be aware of small bowel perforation and obstruction as a not-so-uncommon side effect of vascular endothelial growth factor (VEGF) blocking agents such as bevacizumab and sorafenib.
STOMATITIS OR ORAL MUCOSITIS
Oral mucositis is defined as inflammation of the oropharyngeal mucosa, manifested clinically as oral/throat pain and redness or mucosal ulceration. The term stomatitis is preferred for the mucosal ulceration seen with targeted agents, specifically the mammalian target of rapamycin (mTOR) inhibitors such as everolimus and temsirolimus. The incidence of oral mucositis is very high particularly in patients receiving concurrent chemoradiation therapy for head and neck cancers, approaching nearly 100% (85% grade 3 to 4 toxicity), and for patients receiving high-dose chemotherapy prior to allogeneic or autologous bone marrow transplantation (approximately 90%). The estimated incidence with other chemotherapeutic agents and targeted agents is lower, ranging from 30% to 75%.1,2 Certain agents induce more mucosal damage than others, infusional 5-FU, cytarabine, bleomycin being a few of the cytotoxics that can be associated with >20% incidence of grade 2 to 4 mucositis (Table 19-4). Quite a few of the biologics cause oral symptoms, including mTOR inhibitors everolimus and temsirolimus, epidermal growth factor receptor (EGFR)-targeted agents such as cetuximab and erlotinib and multi-tyrosine kinase inhibitors such as sorafenib, sunitinib, dasatinib, and pazopanib4,5 (Table 19-1). Combination of cytotoxics and chemotherapy or radiation therapy may cause synergistic effects.6
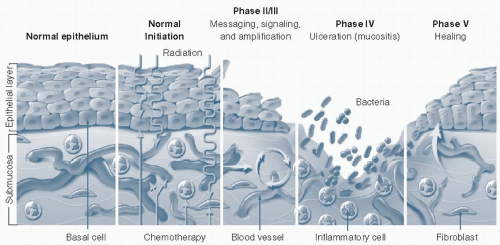
Chemotherapy-induced generalized mucositis can cause oral lesions, dysphagia, odynophagia, dyspepsia, and diarrhea. Mucositis typically manifests 5 to 7 days after starting therapy and may last up to 2 to 3 weeks if secondary to chemotherapy and targeted therapy, but can be prolonged to 6 weeks if secondary to radiation therapy. The pathophysiology of generalized and oral mucositis is similar and is elegantly illustrated in Figure 19.1.3,7 Five steps in the development of mucositis have been described:
Initiation: Damage to DNA and other targets in the cell via reactive oxygen radicals and direct toxicity induced by chemotherapy and radiotherapy (and presumably by targeted therapy).
Primary damage response phase: Nuclear factor-kappa B (NFkB) (along with Wnt, p53, and their associated canonical pathways) is activated and upregulated and further activates the members of the proinflammatory cascade.
Amplification: Via multiple signaling pathways (which are not completely understood), the proinflammatory cascade is amplified several fold with the help of feedback loops. This stage is the precursor of overt clinical mucositis.
Ulceration: Mucosal barrier breakdown results in clinical manifestations ranging from mild erythema to frank ulceration with coalescent pseudomembranes (erosive mucositis). This stage is usually complicated by secondary bacterial infection, which amplifies the process.
Healing: The extracellular matrix (ECM) in the submucosa is the main player in the healing stage, which is usually selflimited.3 The ECM guides the proliferation, migration, and differentiation of the epithelium bordering the ulcer.
Various risk factors have been identified, including drug and drug-specific factors (such as dose, route, and frequency) and patient factors. Chemoradiation for head and neck cancer and myeloablative chemotherapy have the highest risk of mucositis. Cell cycle-specific drugs, such as bleomycin, 5-FU, and methotrexate, have enhanced stomatotoxic effects as do drugs that are secreted in the saliva, such as etoposide and methotrexate. Bolus or prolonged infusions also increase risk. Among the newer targeted agents, EGFR-targeted agents and mTOR inhibitors are associated with higher risk (40%). Table 19-1 shows the chemotherapeutic and targeted agents associated with increased mucositis risk.
Patients with Addison’s disease and psoriasis have increased risk, presumably due to increased epithelial proliferation and proinflammatory cytokines. Genetic factors also play a role and have not been studied extensively. It is well known that patients with deficiency of the enzyme dihydropyrimidine dehydrogenase (DPD) have increased oral and systemic toxicity due to 5-FU and capecitabine.8 Young patients and those with poor dental hygiene have higher risk. It is imperative that patients undergoing (chemo)radiation to the head and neck area and high-dose chemotherapy with stem cell transplant (SCT) have pretreatment dental examination. Caries therapy, root planning and scaling, endodontic therapy, and possible teeth extraction for severe dental disease should be performed prior to treatment.
Clinical practice guidelines for the prevention and treatment of cancer therapy-induced oral mucositis have been established by the Multinational Association of Supportive Care of Cancer (MASCC) in 2004 and last updated in 2007.6,9,10 Although multiple prophylactic drugs and strategies have been explored over the years, including sucralfate, allopurinol, glutamine, chamomile tea, vitamin E, chlorhexidine, antimicrobial lozenges, GCSF rinses and acyclovir, none have shown to prevent mucositis effectively and are not recommended. The only practice that has shown to reduce the incidence of mucositis by about 50% is oral cryotherapy, which is the use of ice chips orally during 5-FU bolus and high-dose melphalan administration.11,12 Oral hygiene is essential, and patients are advised to brush teeth and floss regularly and avoid the use of food that are spicy, salty, rough, and acidic (grapefruit, lemon, and orange).
Figure 19.1 Pathobiology of mucositis: a five-stage process. (Reprinted with permission from Sonis ST. A biological approach to mucositis. J Support Oncol. 2004;2(1):21-32; discussion 35-36.)
An exciting new agent that is now FDA approved for mucositis prevention in high-dose chemotherapy and TBI (total body irradiation) in the autologous SCT setting is palifermin, a keratinocyte growth factor. Intravenous palifermin given 3 days prior and 3 days after the infusion of stem cells significantly decreased grade 3 to 4 mucositis (63% vs. 98%), median duration of mucositis (6 vs. 9 days), use of opioid analgesics, and need for parental nutritional support.13 Although there are several studies demonstrating the benefit of palifermin in treatment of nonhematological malignancies not associated with SCT (5-FU using Mayo clinic bolus regimen, ifosfamide, and high-dose doxorubicin), it is not recommended for routine use as the cost benefit factor is unknown. Also, in the placebo-controlled trial evaluating palifermin in patients receiving 5-FU for metastatic colorectal cancer, oral cryotherapy was not used, and hence absolute benefit in a realistic clinical setting is unproven.14
Two small studies exploring the role of helium-neon low-level laser pretreatment (LLLT) at reducing mucositis in patients undergoing SCT showed some efficacy, but no decrease in the need for parental nutrition.15,16 As only few centers have the ability to administer LLLT, this is not routinely used in clinical practice.
Although there are some data available for the establishment of guidelines in the prevention of mucositis, there is a dearth of reliable data in the realm of treatment, and most strategies are intuitive and make clinical sense.17 The strategies to treat established mucositis include oral care, dietary modifications, analgesics (topical and or systemic) for pain management, and topical mucosal protectants. Patients are advised to brush gently two to three times daily with a soft bristled toothbrush using fluoride toothpaste and to observe gentle flossing. Saline baking soda mouth rinses (½ tsp salt and ½ tsp baking soda in a cup of warm water) are advised for cleansing every 4 hours. Dentures should be removed, specifically at night.2 Dietary modifications as described in the prevention of mucositis (see above) are also used for the management of mucositis. It is particularly stressed to the patient that it is important to avoid smoking and alcohol. Early use of topical and systemic analgesics is recommended for symptomatic relief. Topical analgesics include viscous lidocaine, but the effects are short-lived. Often, topical analgesics are combined with sodium bicarbonate, diphenhydramine, nystatin, tetracycline, hydrocortisone, antacids, and other combinations based on institutional preference (Mary’s Magic Mouthwash), but none of the cocktails have been demonstrated to be superior to the other. When topical agents are ineffective and pain continues to be an issue, oral or parenteral narcotic analgesics are administered. Several formulations that can be given via gastrostomy tube if oral intake is painful, and fentanyl patches can be used for continuous analgesia. It is also important to recognize fungal infections, notably thrush or mucocutaneous candidiasis, which are frequently associated with and can exacerbate oral pain due to mucositis. Thrush should be promptly treated with topical antifungals (nystatin) and if ineffective, systemic therapy with azoles.
Several preparations and drugs are in the pipeline and include zinc, manuka honey, homeopathic medication Traumeel, hyperimmune colostrum, recombinant epidermal growth factor, cucurmin, velafermin, dexpanthenol mouthwash, to name a few (www.ClinicalTrials.gov). It is to be seen if any of these will pan out to be effective in the management of oral mucositis.
DYSGEUSIA
Taste perversion or dysgeusia is a well-known but often underreported oral toxicity associated with many chemotherapeutic and targeted antineoplastic agents, as also radiation to the head and neck area.18 Dysgeusia is a complicated symptom that is difficult for accurate objective assessment and is closely associated with changes in olfaction, and is frequently related to changes in flavor (Table 19-4). Dysgeusia may be related to the underlying malignancy (neurologic compression of olfactory and gustatory nerves), hyponatremia, and several other medicines that are used to alleviate other toxicities of cancer therapeutics (antidepressants and anticholinergics). The exact incidence of dysgeusia is not known, as most studies fail to report this symptom separately from mucositis. Few studies are available, with subjective reports of prevalence of taste disturbances ranging from 44% to 72%.19,20,21 The duration of dysgeusia is unpredictable and may persist for several months after discontinuation of offending drug or radiation. There is a significant deterioration in quality of life, as change in taste perception and flavor frequently results in anorexia, appetite changes, cachexia, and perhaps inferior outcomes from therapy.19,21 Radiation-induced dysgeusia is believed to be secondary to salivary gland dysfunction (causing xerostomia or dry mouth) and direct toxicity to the taste buds. Chemotherapeutic agents that have been most commonly associated with this symptom include cisplatin, carboplatin, etoposide, cyclophosphamide, methotrexate, and taxanes.22 A recent study has also demonstrated an increase in incidence of dysgeusia with irinotecan use.20 Dysgeusia is increasingly recognized as a side effect of targeted antineoplastic treatment, especially with tyrosine kinase inhibitors (TKIs) such as vandetanib, sorafenib, imatinib (25% to 39%), sunitinib, as also with mTOR inhibitors and EGFR-targeted agents.4,23
Zinc deficiency has been postulated to be a major factor in the pathogenesis of dysgeusia, as zinc is a cofactor in alkaline phosphatase metabolism, which is the most abundant enzyme in the taste bud membrane. Data supporting the routine supplementation of zinc are sparse, however. A phase III randomized placebo-controlled trial of 169 patients undergoing chemoradiation for head and neck cancer demonstrated that there was a definite trend to the reduction in the incidence of dysgeusia with the use of 45 mg three times a day of zinc sulfate, but the difference was not statistically significant (84% in zinc treated and 73% placebo arm).24 Amifostine, likewise, did not demonstrate any appreciable therapeutic benefit, in fact, one study demonstrated statistically significant increase in dysgeusia in the treatment arm (32% vs. 10%; P = .039).25 Self-reported patient management strategies include ingestion of cold meals, avoidance of certain “trigger” foods and strong smells, and increased use of seasonings and spice.26 However, literature on the actual efficacy of any of these interventions is scarce and no solid recommendations can be reliably made.
ESOPHAGITIS
Esophagitis can occur as a direct toxicity of chemotherapy or radiation therapy, or it can be secondary to bacterial, fungal, and viral infections following immunosuppression due to chemotherapy. The most common infectious causes include Candida sp., Herpes simplex virus (HSV), Cytomegalovirus, Varicella zoster virus, or polymicrobial oral flora. Acute or chronic graft-versus-host disease (GVHD) is another etiology of esophagitis or diarrhea in patients who undergo allogeneic hematopoietic stem cell transplantation. Patients could also have concomitant gastroesophageal reflux disease (GERD), pill-induced esophagitis (doxycycline use for EGFR-mediated skin reaction), or could be symptomatic with underlying tumor (esophageal invasion of lung cancer, esophageal cancer, and malignant stricture). Chemotherapeutic agents can cause direct cytotoxicity to the esophageal mucosa, and the pathophysiology is believed to be similar to that of oral mucositis.3 However, direct esophageal toxicity is seen mostly when chemotherapy or targeted therapy is used in combination with radiation to the thoracic area.27 Patients frequently present with retrosternal burning, dysphagia, and odynophagia (Table 19-4 for grading system).
The management of esophagitis depends on the clinical scenario. Esophagitis seen in a patient undergoing concurrent chemoradiation to the chest is treated with conservative measures such as hydration, enteral or parenteral nutrition, adequate pain control with patient controlled analgesia, and use of antacid therapy (proton pump inhibitors and H2 blockers). There has been no definite proven benefit in the use of topical lidocaine and institution-based combination regimens such as Mary’s Magic Mouthwash, but these are frequently used in clinical practice. Endoscopy is not commonly utilized in this setting due to the risk of perforation of inflamed friable mucosa; however, it can be of therapeutic and diagnostic benefit if stricture or infection is suspected.
If any suspicious oral lesion is seen that is suggestive of HSV infection, it is likely that esophagitis is also due to the same infection. In this setting, culture of the oral lesion followed by acyclovir therapy is recommended. Acyclovir can be given orally 400 mg orally five times daily × 14 to 21 days or 5 mg per kg intravenously every 8 hours for 7 to 14 days.28 Foscarnet is used in refractory cases.
Candidasis is a more common etiology of infectious esophagitis seen due to immunosuppression from chemotherapy and is usually associated with mucocutaneous features such as oral thrush. Empiric antifungal therapy is recommended; with suspected candida esophagitis, systemic therapy (azoles and echinocandins) is preferred over topical therapy (nystatin).29
CMV esophagitis is a complication observed within 100 days of stem cell transplantation.30 Endoscopy with biopsy is frequently used to differentiate from GVHD; positive serologies also help in the diagnosis. CMV infection is rare, but increasingly seen in nontransplant patients with hematologic malignancies treated with rituximab and steroids, as also other targeted therapies that cause profound T cell immunosuppression.31 Treatment is with ganciclovir or foscarnet.
DYSPHAGIA AND ODYNOPHAGIA
Dysphagia refers to the symptom of difficulty swallowing, and odynophagia implies painful swallowing (Table 19-4 for grading). Although there are numerous causes of dysphagia or odynophagia in the oncologic patient, including tumor effect (upper aerodigestive tract malignancies), paraneoplastic conditions, strictures, pill induced esophagitis, and other causes, they can also be seen as a treatment effect—mainly due to oroesophageal mucositis, and are often associated with concurrent chemoradiation of the head and neck area. Please refer to the mucositis and esophagitis sections in this chapter for further details about pathophysiology and management of dysphagia and odynophagia.
NAUSEA AND VOMITING
Nausea and vomiting are common side effects of chemotherapy and molecular-targeted therapy. With the advent of newer agents used to treat chemotherapy-induced nausea and vomiting (CINV), the incidence has greatly decreased; however, this still continues to be a significant cause of concern to patients (Table 19-4 for grading system). The incidence of acute CINV (within 24 hours of drug administration) is estimated to be 37% to 59% and delayed CINV (>24 hours after administration) occurs in 47% to 75% of patients treated with chemotherapy.32,33 Although emesis appears to be better controlled with the newer antiemetic agents, nausea is still a problem and can adversely affect the patient’s quality of life.33,34,35 Interestingly, delayed CINV is underreported by practitioners when compared with patient reports, which underlines the complex pathophysiology of CINV and the importance of continued efforts toward ameliorating this disabling side effect of chemotherapy.35 CINV can cause decrease in quality of life,34 disruption in treatment schedules, decrease in compliance, medical complications such as dehydration, poor nutrition, electrolyte imbalance, frequently resulting in hospitalization and elevation in the costs of health care and loss of work days.36
CINV can be described as being acute, delayed, or anticipatory. Acute CINV occurs within the first 24 hours of drug administration, with an onset within 1 to 2 hours and typically peaks at 4 to 6 hours. Delayed CINV occurs after the first 24 hours and may persist for up to 1 week. This was first described in 1985 with cisplatin, one of the most emetogenic medications at that time.37 Anticipatory nausea is an interesting conditioned Pavlovian response seen in patients who have previously experienced severe CINV. The triggers could be variable and include environment (physician’s office and infusion room), smells, foods, or even other cognitive stimuli. Anticipatory nausea can occur prior to drug administration or on the same day of subsequent chemotherapy infusion.38 Although acute and anticipatory nausea have decreased in incidence due to improved antiemetic control, delayed CINV continues to be an issue.
There is an increased risk of CINV seen in younger patients and female sex.39 Treatment-related factors are by far more important in causation; the two factors are: chemotherapeutic dose and emetogenecity of the drug.
An initial guide to emetogenecity was published first in 1997 by Hesketh and colleagues,40 which was subsequently modified by an expert consensus panel in 200641 and is now incorporated into various society guidelines for antiemetic treatment, including ASCO, ESMO, and MASCC.
There are four risk levels identified: high (>90%), moderate (30% to 90%), low (10% to 30%), and minimal (<10%), based on the risk of emetogenecity of intravenous chemotherapeutic agents. Of note, this does not take into account the risk of nausea. The initial ASCO guidelines were published in 1999 and last updated in 2006.42 The latest and most comprehensive update is in the form of the results of the third International Perugia Consensus Conference meeting in 2009, published in 2010. For the first time, emetogenecity risks of oral agents were established.43Table 19-2 is an adaptation of the 2006 ASCO guidelines and 2010 ESMO and MASCC guidelines for emetogenecity risk and optimal treatment strategies.
The molecular-targeted agents associated with nausea and vomiting are mainly small molecule TKIs, and include sunitinib, imatinib, lapatinib, erlotinib, sorafenib, dasatinib, and nitotinib. Proteosome inhibitors, such as bortezomib, and mTOR inhibitors, temsirolimus and everolimus, also cause nausea and vomiting. The monoclonal antibodies associated with nausea and vomiting are cetuximab, panitumumab, and tositumomab. The incidence of nausea and vomiting with molecular-targeted agents is highly variable and can range from 18% with sorafenib44 and everolimus to 56% with sunitinib23 and 70% with imatinib.45 Targeted agents can cause more nausea than emesis, for example, sunitinib has approximately 50% incidence of all grade nausea, but only about 25% to 30% incidence of emesis.23
There has been a lot of work done in the past couple of decades toward elucidating the pathophysiology of CINV, which is complex and involves several pathways. Figure 19.2 demonstrates the current understanding of the pathophysiology with involvement of the small intestine and two areas in the brain stem: nucleus tractus solidarus (NTS) and area postrema. The concept of a single “vomiting center” in the brain proposed by Wang and Morison46 in 1950 is now replaced by a complex set of neurons called the “central pattern generator,” believed to coordinate the series of events that lead to emesis, as proposed by Koga and Fukuga47 in 1992. It is now believed that the principal actors are the neurotransmitter receptors for serotonin 5-hydroxy tryptamine3 (5HT3), dopamine, substance P, and cholecystokinin, which are located in the enterochromaffin cells in the small intestinal epithelium and are the terminal ends of vagal afferents. Antineoplastic agents stimulate these vagal afferents either by direct toxicity or by breaking of mucosal barrier and causing the release of neurotransmitters from the enterochromaffin cells, which then bind to the receptors; the stimulus is carried to the dorsal brain stem (NTS and area postrema) and activates the central pattern generator.48 Area postrema contains the chemotherapy trigger zone and may have different mechanisms of activation, which are incompletely understood. The amygdala is another less-understood area of the brain that is associated with CINV. 5HT receptors are found in all three key areas: the vagal afferent chain, NTS, and area postrema. 5HT3 is the most important of all of the receptors in mediating CINV. It is has been shown that the abdominal vagal afferents are the principal mediators of CINV with 5HT3 agonists.49 Although dopamine, 5HT3, and substance P (a neurokinin) all exert pro-emetic effects, endocannabinoids have antagonistic action.50
Each of these neurotransmitters and their receptors are potential targets for development of antiemetic drugs. Dopaminergic antagonists were available prior to the use of cisplatin. Treatment of CINV has improved substantially since the introduction of the 5HT3 antagonists in the early 1990s. There are five approved drugs in this class for use with high to moderately emetogenic antineoplastic agents: ondansetron, granisetron, dolasetron, tropisetron (first generation agents), and the second generation agent palonosetron (40 hours half-life). It has been well established that all the four first generation agents have equivalent efficacy,51 oral formulation is equivalent to intravenous dose, single dose is as efficacious as multiple doses52 and that efficacy is superior in combination with dexamethasone.53 Although the first generation 5HT3 antagonists are quite effective in preventing acute CINV, palonosetron has been shown to decrease delayed CINV as well. Palonosetron has a 30- to 100-fold greater affinity for the 5HT3 receptor and a much longer half-life than the first generation agents. Single-dose palonosetron along with dexamethasone prophylaxis has been shown to prevent acute emesis by 63% to 75% and delayed emesis by 54% to 57%.54,55,56 There is no significant difference between the 0.25 and 0.75 mg dose.54 Although a few studies showed an improved response rate with palonosetron compared with the first generation agents, it is unknown whether the difference in efficacy would still hold with the concomitant use of aprepitant (as practiced clinically for highly emetogenic chemotherapy). Hence, current MASCC guidelines do not recommend one 5HT3 antagonist over another.43
Table 19-2 Emetogenic Potential of Intravenous and Oral Cytotoxics and Biologic Antineoplastic Agents
Degree of Emetogenicity (Incidence)
Drug
Cytotoxics
Biologics
High (>90%)
IV
Cisplatin
Mechlorethamine
Streptozotocin
Cyclophosphamide (≥ 1,500 mg/m2)
Carmustine
Dacarbazine
None
Oral
Procarbazine
None
Moderate (30%-90%)
IV
Oxaliplatin
Cytarabine >1 g/m2
Carboplatin
Ifosfamide
Cyclophosphamide <1.5 g/m2
Doxorubicin
Daunorubicin
Epirubicin
Idarubicin
Irinotecan
Bendamustine
Clofarabine
Azacitidine
Alemtuzumab
Oral
Cyclophosphamide
Temozolomide
Vinorelbine
Imatinib
Low (10%-30%)
IV
Paclitaxel
Docetaxel
Cabazitaxel
Mitoxantrone
Doxorubicin HCl liposomal Injection
Ixabepilone
Topotecan
Etoposide
Pemetrexed
Methotrexate
Mitomycin
Gemcitabine
Temsirolimus
Bortezomib
Cetuximab
Trastuzumab
Panitumamab
IV
Cytarabine ≤ 1 g/m2
5-Fluorouracil
Oral
Capecitabine
Tegafur Uracil
Fludarabine
Etoposide
Sunitinib
Everolimus
Lapatinib
Lenalidomide
Thalidomide
Minimal (< 10%)
IV
Bleomycin
Busulfan
2-Chlorodeoxyadenosine
Fludarabine
Vinblastine
Vincristine
Vinorelbine
Bevacizumab
Cetuximab
Oral
Chlorambucil
Hydroxyurea
L-Phenylalanine mustard
6-Thioguanine
Methotrexate
Gefitinib
Erlotinib
Sorafenib
Note: Degree of emetogenicity refers to total percentage of grade 3 to 4 nausea and emesis as reported in clinical trials. IV, intravenous. Adapted from ASCO and ESMO guidelines for management of nausea and vomiting due to antineoplastic agents.42,43
In the past decade, there have been several randomized trials conducted with newer antiemetic agents, but none have panned out to be as efficacious as the relatively new class of agents called the neurokinin inhibitors (NK-1), which have been clinically available since 2003. Aprepitant (and the intravenous watersoluble prodrug fosaprepitant) has been the most used in clinical practice; casopitant is another potent and selective NK-1 inhibitor that has been studied in clinical trials, but no longer available. The NK antagonists selectively block substance P from binding to the NK-1 receptor in the CNS, presumably at the NTS and area postrema (Fig. 19.2).57
The efficacy of aprepitant in preventing CINV (both acute and delayed) with highly emetogenic chemotherapy has been well established. Three large phase III studies demonstrated that aprepitant in combination with a 5HT3 antagonist and dexamethasone reduced the incidence of acute CINV from 43%-63% to 63%-73%, when compared with 5HT3 antagonist and dexamethasone alone; all studies demonstrated high statistically significant differences.58,59,60 Both aprepitant and fosaprepitant are FDA approved for 3-day dosing, with aprepitant administered as 125 mg on Day 1 and 80 mg orally on Days 2 and 3. As of 2010, fosaprepitant is no longer available in the 115 mg strength and hence is administered as a single dose of 150 mg prior to chemotherapy. This is considered equivalent to the 3-day dosing.61
Aprepitant62 inhibits cytochrome P450 enzyme 34A and induces CYP2C9. Hence, the dose of dexamethasone is reduced by 40% to 50%. In all the phase III studies, dexamethasone was reduced from 20 to 12 mg pre-chemo and dexamethasone taper was reduced from 8 mg twice a day to 8 mg daily.58,59,60 Although a large number of drugs (including taxanes, etoposide, irinotecan, ifosfamide, imatinib, and vinca alkaloids) could theoretically have altered metabolism and or efficacy with NK1 antagonists, the few drug interaction studies conducted do not demonstrate any problems at the clinically used doses.63,64,65 It is recommended that INR be closely monitored with concomitant warfarin use and that patients be counseled about the potentially reduced efficacy of oral contraceptive pills.64,65
Figure 19.2 Pathophysiology of emesis. (Reprinted with permission from Hesketh PJ. Chemotherapy-induced nausea and vomiting. N Engl J Med. 2008;358(23):2482-2494.)
The antipsychotic drug olanzapine also appears to have activity against CINV, particularly delayed nausea. An initial phase II trial conducted by the Hoosier Oncology Group utilizing a combination of olanzapine, palonosetron, and dexamethasone with highly and moderately emetogenic chemotherapy demonstrated 100% response rate in acute emesis, and 75% with delayed emesis.66 It was intriguing that nausea was also controlled by 100% in the acute setting and 50% in the delayed setting. This has been confirmed in a phase III trial of 50 patients receiving cisplatin or doxorubicin and cyclophosphamide (preliminary report presented as an abstract in ASCO 2010) comparing 10 mg olanzapine (days 1 to 4) with palonosetron and dexamethasone versus aprepitant with palonosetron and dexamethasone. Although the rates of acute and delayed emesis control were similar (and comparable with previous studies), an interesting finding was that delayed nausea was reduced to 67% in the olanzapine arm versus 38% in the aprepitant arm.67 Final results of this study are awaited prior to changing current practice guidelines for the use of olanzapine in CINV.
Ginger has also been studied in CINV. Although a recent placebo-controlled randomized study with ginger administered for 6 days (3 days prior to chemotherapy) suggested that ginger was successful in preventing chemotherapy-induced nausea,68 the benefit appeared to be lost when ginger was combined with aprepitant and/or 5HT3 antagonist.69 There currently does not appear to be a role for ginger in CINV. Alternative therapies such as acupuncture, exercise, hypnosis, and systematic densentization have been evaluated in randomized controlled studies,70 but all of them appear to have limited benefit and are not routinely recommended.
Anticipatory nausea is a behavioral response to a previous ill-tolerated chemotherapeutic or targeted treatment and is believed to occur in 25% of patients by the fourth treatment cycle. There has been a recent decline in anticipatory CINV, with the rate of anticipatory nausea believed to be <10% and emesis to be <2%.43,71 The reason for the decline in prevalence has been attributed to the advent of 5HT3 antagonists and NK1 antagonists. Certain patient characteristics such as age <50 years, susceptibility to motion sickness, anxiety personality, nausea and vomiting with the previous chemotherapy cycle, history of sweating with the previous treatment, all predict toward development of anticipatory nausea and emesis.72 Once anticipatory nausea occurs, it may be difficult to treat. Benzodiazepines are the only pharmacologic agents proven to have a benefit in this setting. A double-blinded placebo-controlled study of 57 patients with 0.5 to 2 mg of alprazolam per day along with psychological support program demonstrated a reduction in anticipatory nausea from 18% to 0% (P = .038).73 Another randomized trial demonstrated that lorazepam significantly reduced the incidence of acute, delayed, and anticipatory nausea induced by high doses of cisplatin.74 Nonpharmacologic techniques include behavioral techniques such as progressive muscle relaxation training, hypnosis, and biofeedback.75 The overall superior management strategy is in preventing anticipatory nausea by better primary control of CINV.
Breakthrough nausea and vomiting, which is persistent nausea and vomiting that occurs in spite of prophylaxis, frequently poses a challenge. It is important to evaluate for and carefully exclude other causes of nausea, such as CNS metastases, bowel obstruction, volume depletion and electrolyte imbalance, uremia, or gastroparesis. If no other organic etiology can be determined, then this is attributable to poor prophylactic control. Medications to manage breakthrough nausea include dopaminergic antagonists (prochlorperazine and haloperidol), benzodiazepines (lorazepam or alprazolam), endocannabinoids (dronabinol), substituted benzamides (metoclopramide), and antipsychotics (olanzapine). Switching to another 5HT3 antagonist (in the same or different class) for the subsequent treatment cycle may be effective.76 For persistent breakthrough nausea, scheduling antiemetics (see above) for round-the-clock coverage may be more effective than as needed (prn) doses. It is helpful to use multiple classes of medications for more effective therapy.
LIVER FUNCTION ABNORMALITIES
Please refer to the hepatoxicity of chemotherapeutic agents, chapter 20, for etiology, pathophysiology, diagnosis, and management.
ENTEROCOLITIS
Chemotherapeutic agents and biologics can induce enterocolitis in an infectious and noninfectious manner. Infectious colitis is most commonly associated with Clostridium difficile infection. The etiology is multifactorial, including immunosuppression from chemotherapy,77 increased hospitalization and antibiotic use due to frequent infections in this population, advanced age, and interestingly, frequent use of proton pump inhibitors.78 Although antibiotic-associated C. difficile infection is the most common etiology, there have been several case reports of chemotherapy-induced C. difficile colitis, the reported inciting agents being: 5-FU, carboplatin, paclitaxel, vinorelbine, methotrexate, and cisplatin.79,80,81,82 Treatment is in analogous to nonchemotherapy-associated infections, with the use of oral metronidazole 500 mg three times daily for 14 days as first-line therapy.
Noninfectious enterocolitis manifests as typhlitis (neutropenic enterocolitis), ischemic enterocolitis, or immune-mediated enterocolitis seen with new biologics such as ipilimumab. Typhlitis is a complication initially described in children receiving induction chemotherapy for leukemia,83 but is now increasingly recognized in adults who develop prolonged and profound neutropenia, mostly related to treatment for acute leukemia, stem cell transplantation, and is also associated with multiple myeloma, myelodysplasia, cyclic neutropenia, and AIDS.84 Although the true incidence of typhlitis is unknown, there are increasing reports of this complication in adults with solid malignancies such as breast, lung, and peritoneal cancer.85,86 The pathophysiology is believed to be centered on mucosal damage by chemotherapy, with profound neutropenia and impaired immunity resulting in bacterial colonization and invasion.87 Diagnosis is usually established by history, exam, and radiologic findings. The suspicion is high in a severely neutropenic patient (absolute neutrophil count <500 per µl), who presents with fever and abdominal pain, maybe associated with nausea, abdominal distension, watery, or bloody diarrhea. Exam may suggest acute findings of peritonitis. CT scan is the preferred imaging modality, and frequently reveals distended dilated cecum, with diffuse cecal wall thickening; occasionally with intramural air, localized peritonitis, or adjacent abscess formation. Mortality can be fairly high (reports up to 45%) and management should be initiated rapidly. Conservative approach is attempted initially, with use of intravenous antibiotics, bowel rest, hydration, and correction of coagulopathy (if present).88 Granulocyte colony stimulating factor can be used to hasten neutrophil recovery.89 Emergent surgical intervention is indicated in uncontrolled GI hemorrhage, perforation, obstruction, or with clinical deterioration. Differentials include ischemic bowel and pseudo membranous enterocolitis associated with C. difficile infection.
Only gold members can continue reading. Log In or Register to continue