Acquired erythrocyte fragmentation occurs when red cells are forced at high shear stress through partial vascular occlusions or over abnormal vascular surfaces.
In circumstances in which fragmentation of red cells occurs in the microcirculation, it is often referred to as microangiopathic hemolytic anemia.
In three primary disorders—thrombotic thrombocytopenic purpura (TTP) (Chap. 90), hemolytic uremic syndrome (HUS) (Chap. 90), and disseminated intravascular coagulation (DIC) (Chap. 85)—microangiopathic (fragmentation) hemolytic anemia is an essential diagnostic feature. These disorders are discussed in other chapters.
In addition to signs of hemolysis such as anemia, reticulocytosis, decreased haptoglobin, elevated indirect bilirubin, and sometimes elevated serum lactic dehydrogenase, fragmented red cells (schistocytes) are evident in the blood film (Figure 19–1). Their prevalence may vary.
Fragmentation hemolytic anemia syndromes discussed in this chapter include (1) hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome, (2) disseminated malignancy, (3) heart valve hemolysis, (4) march hemoglobinuria, and (5) the Kasabach-Merritt phenomenon.
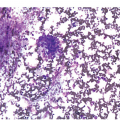
FIGURE 19–1
This image shows typical appearance of fragmented red cells. Two cases of fragmentation hemolytic anemia as a result of heart valve hemolysis. The red cell shape abnormalities are varied and characteristic of fragmentation hemolysis, although they are not specific for the cause. In the normal blood film, cells that deviate significantly in form from the normal circular shape occur only once every several thousand cells. The average oil immersion field in an area suitable for examining red cell morphology contains approximately 200 red cells. In a patient with anemia, that number may be much less. Thus, even one fragmented cell per oil immersion field is notable, although not in itself diagnostic. (Reproduced with permission from Lichtman’s Atlas of Hematology, www.accessmedicine.com.)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


