XI.A.001 Acute Hemorrhagic Edema of Infancy

XI.A.001
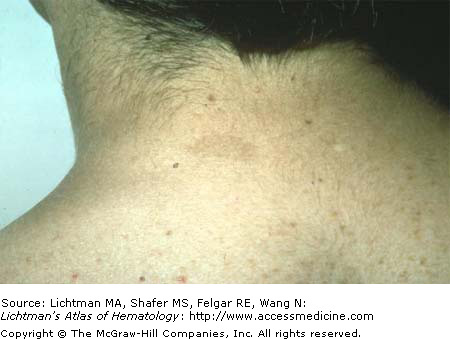
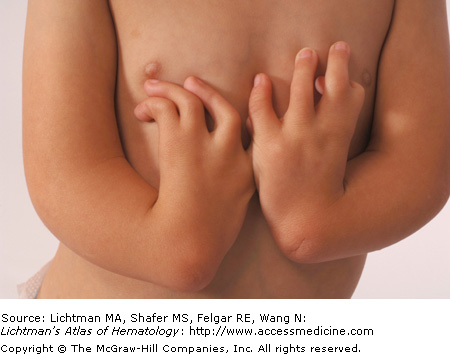
Acute hemorrhagic edema of infancy is an acute cutaneous leukocytoclastic vasculitis (LCV) of infants with a violent onset followed by spontaneous recovery. Edema and palpable purpuric skin lesions are present. Light microscopic examination of the skin biopsy specimens revealed LCV as in Henoch-Schönlein purpura. Acute hemorrhagic edema of infancy is observed before 2 years of age and is confined to the skin.
XI.A.002 Amyloidosis, Primary

XI.A.003 Amyloidoses, Primary
XI.A.004 Antiphospholipid Antibody Syndrome

XI.A.005 Antiphospholipid Antibody Syndrome: Lupus Anticoagulant
XI.A.006 Aspergillosis

XI.A.006
Aspergillosis: primary cutaneous lesion initiated from a contaminated arm-board. Primary cutaneous aspergillosis can occur in the absence of disseminated disease. In hospitalized patients, primary cutaneous aspergillosis lesions may arise around the sites of an intravenous catheter or a venipuncture site.
XI.A.007 Candidiasis, Disseminated

XI.A.007
Disseminated candidiasis. Purpuric nodule and diffuse maculopapular and maculonodular rash in a patient with acute myelogenous leukemia with invasive (disseminated) candidiasis. The rash of candidiasis may be diffuse or only on the extremities. Biopsy, which includes the involved areas down to the dermis will show small oval blastospores with buds and pseudohyphae.
XI.A.008 Chediak-Higashi Disease

XI.A.009 Chediak-Higashi Disease

XI.A.009
Chediak-Higashi disease. Normal and affected mink. The latter (on the right) has light gray hair and absence of pigment in the irises, which appear translucent. The affected child usually has similar findings. The pigment abnormality is the result of misdistribution of abnormal giant melanophores.
XI.A.010 Cholesterol Emboli

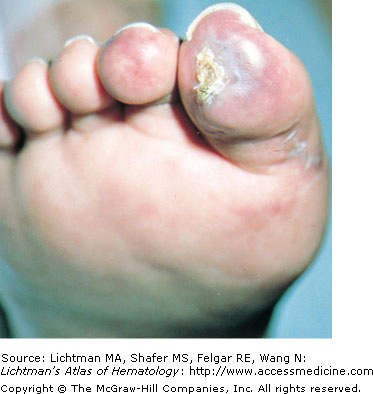
XI.A.010
Cholesterol emboli. Digital necrosis. Small cholesterol crystals or larger cholesterol plaques break off from atherosclerotic plaques and shower into the arterial system, occluding arterioles or larger vessels. Virtually any organ can be affected depending on the size of the crystal or plaque dislodged. The crystals or plaques and an accompanying inflammatory reaction and adventitial fibrosis obliterate the vessel lumen. Vasospastic mediators may contribute to ischemia and necrosis.
XI.A.011 Cholesterol Emboli

XI.A.012 Congenital Rubella

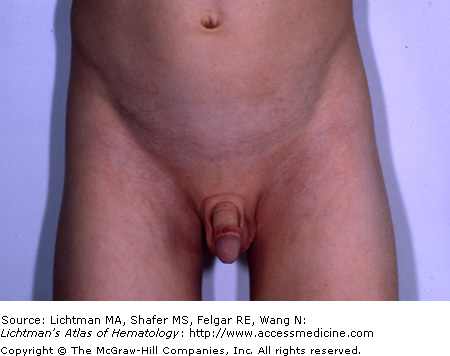
XI.A.012
Congenital rubella. Rare in industrialized societies as a result of rubella immunization. Rubella virus transmitted as a result of maternal infection during pregnancy. Cutaneous manifestation characterized by widespread maculopapular lesions of a reddish-blue or magenta color, due to persistent dermal extramedullary erythropoiesis in patients with congenital viral infections. This circumstance is referred to as blueberry muffin baby.
XI.A.013 Coumadin Necrosis of Breast



XI.A.016 CREST Syndrome

XI.A.016
CREST syndrome is a form of systemic sclerosis (scleroderma) that is characterized by Calcinosis (calcium deposits), usually in the fingers; Raynaud; loss of muscle control of the Esophagus, which can cause difficulty swallowing; Sclerodactyly, a tapering deformity of the bones of the fingers; and Telangiectasia, small red spots on the skin of the fingers, face, or inside of the mouth.
XI.A.017 Cryocrystalglobulinemia, Skin Alterations
XI.A.017
Cryocystalglobulinemia. Skin alterations. Woman with a circulating monoclonal immunoglobulin that crystallized at ambient temperatures resulting in ischemic changes in the vasculture of the skin. She developed chronic necrotic lesions with ulceration. See also VII.C. under “Cryocrystalglobulinemia” for images of intravascular crystals.
XI.A.018 Cryoglobulinemia

XI.A.018
Cryoglobulinemia: purpura in this case. Skin manifestations may include ischemic necrosis; palpable purpura; livedoid vasculitis; cold-induced urticaria; scarring of the tip of the nose, pinnae, fingertips, and toes; acrocyanosis; or nailfold capillary abnormalities. Type I cryoglobulinemia, or simple cryoglobulinemia, is the result of a monoclonal immunoglobulin, usually immunoglobulin M (IgM). Types II and III cryoglobulinemia (mixed cryoglobulinemia) contain rheumatoid factors, which are usually IgM. The rheumatoid factor may be monoclonal (in type II cryoglobulinemia) or polyclonal (in type III cryoglobulinemia) immunoglobulin. Cryoglobulinemia without an associated disease has been known as essential, or idiopathic, cryoglobulinemia. However, the discovery of a close association between hepatitis C virus and mixed cryoglobulinemia has cast doubt on the existence of essential, or idiopathic, cryoglobulinemia. Cryoglobulinemia associated with a particular disease (lymphoproliferative disorder, autoimmune disease, infectious disease) is known as secondary cryoglobulinemia.

XI.A.020 Cullen Sign

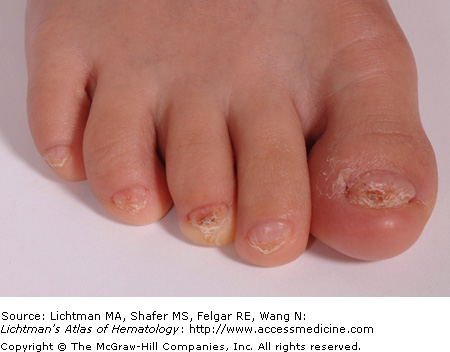
XI.A.021 Dyskeratosis Congenita, Toenails
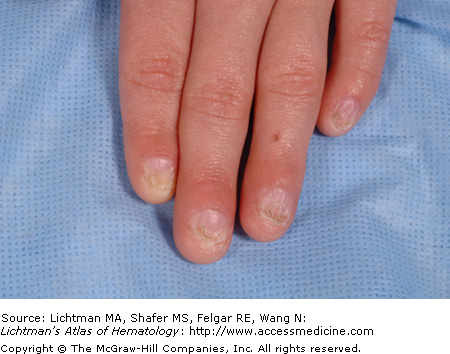
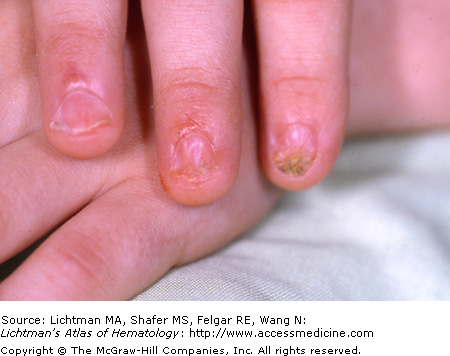
XI.A.022 Dyskeratosis Congenita, Fingernails
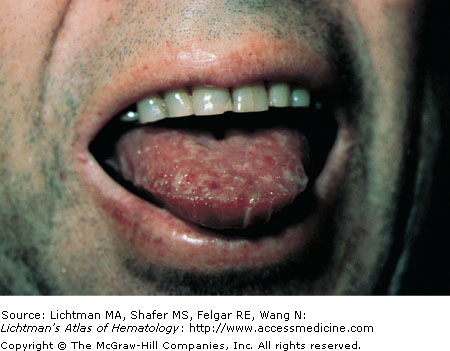
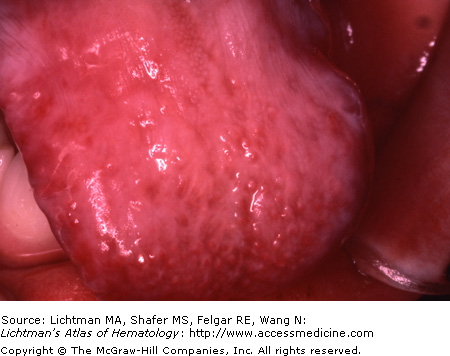
XI.A.023 Dyskeratosis Congenita, Tongue
XI.A.024 Dyskeratosis Congenita, Fingernails
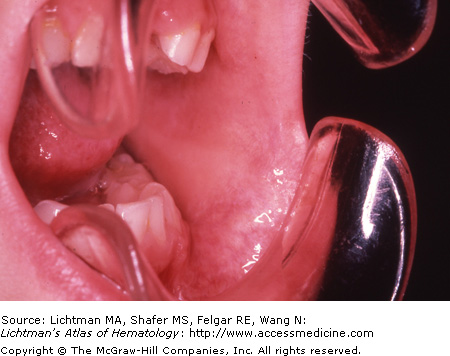
XI.A.025 Dyskeratosis Congenita, Oral Cavity
XI.A.026 Dyskeratosis Congenita, Skin of Groin
XI.A.027 Ecthyma Gangrenosum

XI.A.028 Ehlers-Danlos Syndrome
XI.A.029 Erythema Multiforme

XI.A.030 Fifth Disease (Parvovirus B-19 Infection)

XI.A.030
Fifth disease (parvovirus B-19 infection). Fifth disease, the result of parvovirus B-19 infection, causes a rash that occurs most commonly in children but can occur in non-immune adults. The manifestation is a “slapped-cheek” rash on the face and a lacy red rash on the trunk and limbs. Occasionally, the rash may itch. Associated with a low-grade fever, malaise, or a “cold” a few days before the rash breaks out. The rash resolves in 7 to 10 days.
XI.A.031 Fanconi Anemia
XI.A.032 Fanconi Anemia

XI.A.033 Fanconi Anemia
XI.A.034 Fanconi Anemia
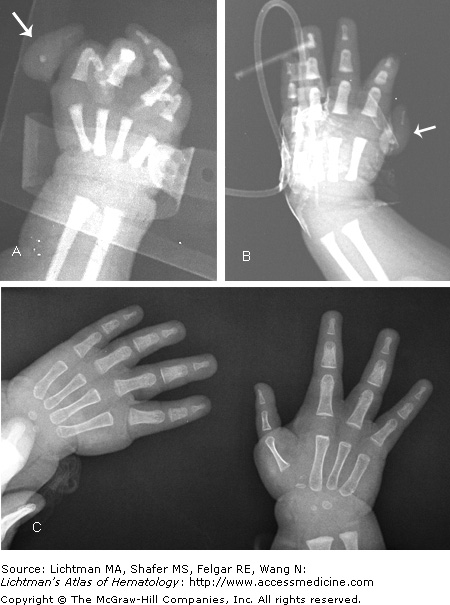
XI.A.034
Fanconi anemia. Radiographs. Vestigial (hanging) thumbs attached by soft tissue. (A) Arrow indicates thumb soft tissue with absence of metacarpal or phalangeal bones in right thumb. (B) Arrow indicates thumb soft tissue with absence of metacarpal or phalangeal bones in left thumb. (C) Left side shows left hand after excision of vestigial thumb (soft tissue removed). Both hands had thumb soft tissue excised. Right side shows right hand after pollicization. The index finger was swung over and an opposable new thumb fashioned, leaving three fingers and new thumb. Left hand had same procedure to provide an opposable thumb (not shown).
XI.A.035 Graft versus Host Disease

XI.A.036 Grey-Turner Sign

XI.A.037 Hemophilia Arthropathy (Factor VIII Deficiency)

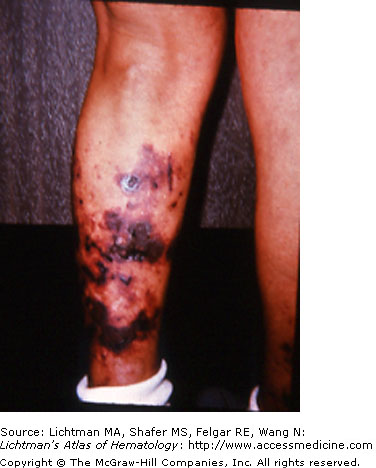
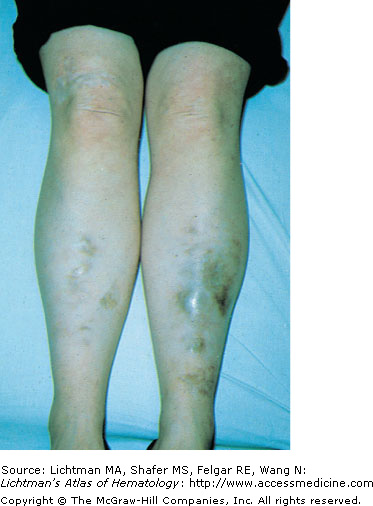
XI.A.037
Hemophilia arthropathy (factor VIII deficiency). Chronic right knee hemarthrosis with fresh and fading ecchymoses on legs. The most common clinical manifestation of hemophilia is arthropathy secondary to recurrent hemarthroses and chronic synovitis. Joint-surface erosions secondary to chronic synovitis often occur in early childhood and progress to advanced arthropathy by late adolescence. The knee, elbow, ankle, hip, and shoulder are the most commonly involved joints.
XI.A.038 Hemophilia Arthropathy (Factor VIII Deficiency)

XI.A.038
Hemophilia arthropathy (factor VIII deficiency). Acute right elbow hemarthrosis with overlying ecchymosis. The most common clinical manifestation of hemophilia is arthropathy secondary to recurrent hemarthroses and chronic synovitis. Joint-surface erosions secondary to chronic synovitis often occur in early childhood and progress to advanced arthropathy by late adolescence. The knee, elbow, ankle, hip, and shoulder are the most commonly involved joints.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


