Differentiating Agents
Bruce A. Chabner
One of the most obvious yet most poorly understood features of malignancy is the apparent failure of cancer cells to differentiate. Malignant cells have the morphologic features of primitive precursors and carry surface markers suggesting that they are blocked at an early step in their maturation. Within this relatively primitive population are cells that preserve the surface antigens (CD38+, CD133−) and biological features of stem cells; like their normal counterparts, they carry the potential for continuous proliferation and tissue renewal. It is speculated that these tumor stem cells are responsible for the long-term survival and growth of clinically apparent tumors and may manifest biological features of drug resistance as found in stem cells of physiological origin.1,2 Thus, it is not surprising that research efforts have turned to the elucidation of factors responsible for the block in tumor cell differentiation, and the identification of agents capable of overcoming this hurdle.
From these inquiries has come one highly effective agent, all-trans retinoic acid (ATRA; Fig. 23-1), that fits the paradigm of a differentiating agent, as it attacks the essential maturation block in acute promyelocytic leukemia (APL). Its key features are presented in Table 23-1.
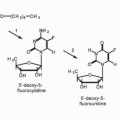
The critical genetic lesion in APL is created by the translocation and regulatory dysfunction of the retinoic acid receptor alpha (RAR-α), a lesion corrected by ATRA. A second treatment for APL, arsenic trioxide (ATO), will also be considered in this chapter. It induces differentiation of APL cells in the clinical setting, although the mechanism of its action remains speculative. Other agents possess differentiating activities and include cytotoxics such as hydroxyurea, 5-azacytidine, decitabine, and cytarabine as well as steroid hormones, including vitamin D and its analogues and corticosteroids, but the relevance of differentiation to their antitumor actions is not well established (see relevant chapters of this book).
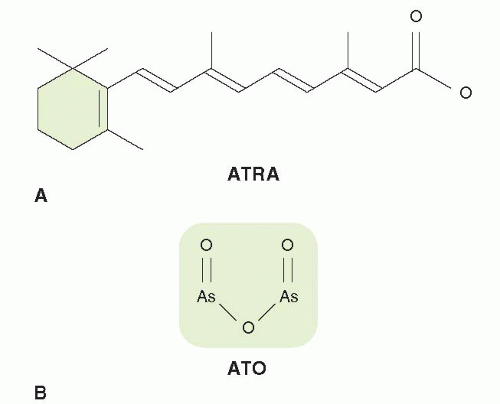 FIGURE 23-1 Structures for PPCC differentiating agents. |
TABLE 23.1 Key features of ATRA | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
All-trans Retinoic Acid
Sporn and colleagues found that retinoids induced differentiation of the human leukemia cell line HL-60 and reversed preneoplastic changes in murine models of epithelial carcinogenesis.3 However, the first successful clinical trials of a retinoid to treat cancer were reported by Wang, Chen, and colleagues from Shanghai in 1988,4 when they described induction of complete remission by ATRA in APL patients refractory to standard chemotherapy. They were aware of Sporn’s earlier work, although the specific involvement of the retinoic acid receptor in APL had not been elucidated at the time of their search for noncytotoxic therapies for acute leukemia.5 Subsequent trials showed that ATRA was able to reverse the often fatal coagulopathy (disseminated intravascular coagulation) associated with APL and that in combination with anthracyclines, it produced long-term recurrence-free survival in the majority of such patients. It is now a standard component of the regimen for remission induction and consolidation therapy for APL.6 Its key features are shown in Table 23-1.
Mechanism of Action
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


