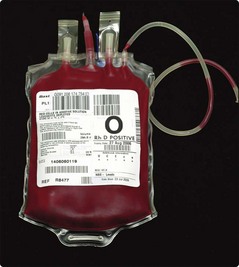
42 Two questions need to be answered before transfusion of red cells is undertaken: Some general indications for red cell transfusion are listed in Table 42.1. Table 42.1 Major indications for red cell transfusion Other haemorrhage (e.g. gastrointestinal bleed) Marrow failure (e.g. aplastic anaemia, leukaemia) Haemoglobinopathies (e.g. thalassaemia, sickle cell disease) Chronic disorders (e.g. renal failure, malignancy) All those involved in the prescription and administration of blood should follow local guidelines with respect to patient identification and the checking of the compatibility and viability of the transfused units. Critical information is contained on the blood bag and the attached compatibility label (Fig 42.1). No discrepancies are permissible. Most serious adverse transfusion reactions are due to transfusion of the wrong blood to the patient (Fig 42.2). Errors can be reduced by newer technologies such as bar coding and radiofrequency chips – these generally rely on machine readable data on patient wristbands. Fig 42.2 Serious hazards of transfusion, United Kingdom 1992–2010 (data with permission of SHOT).
Clinical practice
Red cell transfusion
Practicalities of red cell transfusion
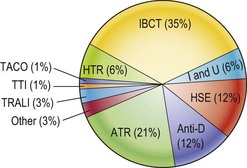
IBCT, incorrect blood transfused; ATR, acute transfusion reactions; HSE, handling and storage errors; I and U, inappropriate/unnecessary/delayed transfusions; HTR, haemolytic transfusion reactions; TRALI, transfusion-related acute lung injury; TACO, transfusion-associated circulation overload; TTI, transfusion-transmitted infections.
Clinical practice