Clinical governance
“Thou wilt learn one piece of Humility, viz. not to trust too much on thine own judgement.” Richard Wiseman ( Severall Chirurgicall Treatises , 1676)
We are in the third health revolution. The first was the arrival of technology to improve care, the second the impact of financial constraints and the third the era of accountability. The measurement and regulation of clinical activity is here to stay.
The key points of clinical governance are to improve clinical care, avoid risk and detect adverse events rapidly. We can influence these by continued professional development, quality improvement, risk management and clinical effectiveness.
There is ample evidence that doctors left to their own devices are not as effective as they would like to think they are, and never have been. Most surgeons would agree that unacceptable variations in standards of care and outcomes must be made to disappear yet, despite good intentions, therapeutic activity that is ineffective or unsubstantiated may take many years to disappear from clinical practice. In addition, our individual practice and the interventions that we use inevitably reflect the current fashion, sometimes in the absence of any evidence base. In contrast, we should not lose sight of the fact that the ‘evidence base’ and systematic reviews may be adversely affected by subjective analysis, interpretations of variations in the results from previous studies, publication bias and missing data. In ideal circumstances, from an idea and hypothesis that leads to technical advances in surgery there should be systematic progression that ends in the development and assessment of appropriate outcome measures. This certainly applies to the development of minimally invasive surgery of the thyroid and parathyroid glands. Are mortality and readmission rates, complications and duration of hospital stay sufficient to show that the new is an improvement on what has gone before?
Examination of new and old controversies in endocrine surgery as shown below tells us that there is currently little evidence to support a rigid approach to how we advise our patients. For example:
Thyroid disease
- •
Do all patients with retrosternal goitre require surgery?
- •
Radioiodine or surgery for patients with thyrotoxicosis?
- •
The extent of surgery for differentiated thyroid cancer?
- •
Prophylactic lymph node dissection in papillary thyroid cancer?
- •
The extent of lymph node surgery in medullary thyroid cancer?
- •
When to complete primary surgery/re-operate in patients with medullary thyroid cancer?
- •
Intraoperative neuromonitoring?
Parathyroid
- •
The indications for surgery in patients with mild hypercalcaemia?
- •
What are the indications for re-operative parathyroid surgery?
- •
Which imaging studies are appropriate prior to re-operative surgery?
- •
What is the role of minimally invasive surgery?
Adrenal
- •
Transperitoneal or retroperitoneal laparoscopic surgery?
- •
Open or laparoscopic surgery in patients with Stage 1 or 2 adrenocortical cancer?
- •
What size of incidentaloma should be removed?
- •
The indications for surgery in subclinical Cushing’s?
- •
Partial adrenalectomy in familial disease?
Pancreas
- •
Which preoperative localisation/regionalisation studies are required in patients with insulinoma/gastrinoma?
- •
When to operate on the pancreas and the extent of surgery in patients with multiple endocrine neoplasia type 1 (MEN1)?
In endocrine surgery there will never be evidence based on prospective randomised controlled trials to support much of what we do, yet should we practise our craft in the manner that our peers have demonstrated to be the most effective? Critical review of our current practice will benefit our patients prior to, during and after surgery.
Various international guidelines, consensus/positional statements are available to guide good practice in the investigation and surgical treatment of adult and paediatric thyroid (thyrotoxicosis, benign nodules, differentiated and medullary thyroid cancer ), parathyroid (hyperparathyroidism ) and adrenal (incidentaloma, malignant tumours ) disease.
Guidelines should help us make decisions about what is appropriate and, in association with a review of whatever evidence there is, lead to change and improvement in patient care. It should be remembered that guidelines are ‘explicit’ information that helps us to make decisions, but the art of medicine needs as much ‘tacit’ as ‘explicit’ input. Written statements describing the rules, actions and conditions that direct patient care can be considered as a medical definition of standards of care.
For the moment we need to stick to guidelines while remembering that they should be part of an iterative process of regular criticism and review, and that they will often need to be adapted to local circumstances. They should ideally be constructed to avoid a dogmatic approach as to what are ‘appropriate’ treatments.
What is good practice?
Clinical governance and quality are synonymous with achieving and maintaining good practice. As there are few, if any, emergencies in endocrine surgery, endocrine surgeons have ample time before any elective intervention to ask:
- •
Which biochemical/cytological tests and imaging studies are necessary prior to surgery, and will their results alter the management of the patient?
- •
Is an operation required? What is the purpose and aim of the procedure? How will this benefit the patient?
- •
Which operation is appropriate in this specific case?
- •
Does the patient understand the indications, implications and risks of surgery in order to give informed consent?
Who should perform surgery on the endocrine glands?
The 1996 consensus statement on thyroid disease by the Royal College of Physicians of London and Society of Endocrinology stated: ‘each District General Hospital should have access to an experienced thyroid surgeon’. Although surgery of the endocrine glands is currently the scene of dispute between general surgeons (endocrine/upper gastrointestinal/hepatobiliary), head and neck, oromaxillofacial, ENT surgeons and urologists, no individual group has an unassailable right to care for and treat the patients. The needs of the patient must come first. The introduction to the British Association of Endocrine and Thyroid Surgeons (BAETS) guidelines states:
“[the guidelines do] not define an endocrine surgeon or specify who should practice endocrine surgery … Elective endocrine surgery will not be in the portfolio of every District General Hospital, but where it is, based on experience and caseload, it should be in the hands of a nominated surgeon with an endocrine interest. Those patients requiring more complex investigation and care as detailed in the guidelines should be referred to an appropriate centre. These rare and complex diseases will only be managed effectively by multidisciplinary teams in Units familiar with these disorders … this category includes patients with endocrine pancreatic tumours, adrenal tumours, thyroid malignancy especially medullary thyroid carcinoma, familial syndromes and those requiring reoperative thyroid and parathyroid surgery.”
The advantages of subspecialisation
It is all too easy to lose sight of the important issues:
- 1.
The surgeon should have been appropriately trained.
In the UK, the higher surgical trainee who declares an interest in endocrine surgery should spend at least 1 year in an approved unit, which should consist of:
- •
one or more surgeons with a declared interest in endocrine surgery;
- •
an annual operative workload in excess of 50 cases (verified by BAETS audit);
- •
on-site cytology and histopathology services;
- •
at least one consultant endocrinologist on site, holding one or more dedicated endocrinology clinics per week, with joint clinics or formal meetings held not less than once per month;
- •
a Department of Nuclear Medicine on site;
- •
on-site magnetic resonance imaging (MRI) and computed tomography (CT) scanning.
In practical terms flexible rotations between regions may be required for more specialised areas of endocrine practice, such as adrenal surgery.
The current syllabus ( www.iscp.ac.uk/documents/syllabus_GS_2010.pdf ) and subspecialist curriculum ( www.baes.info/Pages/BAETS%20Guidelines.pdf ) for endocrine surgical training in the UK are well defined. Examples of how endocrine surgical operative experience and competence for an individual trainee can be identified and rated ( www.nthst.org.uk/Assets/Files/RITA_forms/NTHST_OpComp_Endocrine_v_1.doc ) are available, and in future will help define what constitutes ‘appropriately trained’.
- 2.
The surgeon must be part of an experienced multidisciplinary team .
Complication rates following thyroid, parathyroid and adrenal procedures are higher in patients treated by non-specialists, and lower when ‘high-volume’ surgeons operate or patients are treated in high-volume centres. This is also true for paediatric endocrine surgery. Supervised trainees and newly established endocrine surgeons can perform thyroid surgery safely.
The care of patients with thyroid cancer should be the responsibility of a specialist multidisciplinary team (MDT) that comprises surgeon(s), endocrinologist and oncologist (or nuclear medicine physician) with support from pathologist, medical physicist, biochemist, radiologist and clinical nurse specialist. All should have expertise and interest in the management of thyroid cancers and show commitment to continuing education in the field.
There is evidence from the UK and the USA to support a continued need for subspecialisation in endocrine surgery and adherence to good practice, e.g. total thyroidectomy and lymph node dissection is the standard of care in patients with medullary thyroid cancer (MTC) yet 10–15% of patients with MTC undergo less than total thyroidectomy and 30–40% of patients have no cervical node dissection. MTC is rare; all patients should be referred for surgical treatment to a cancer centre.
- 3.
As the quality of the care received by the patient is paramount it should be subject to assessment by audit and benchmarking against agreed standards .
In 1998, a retrospective study from a single district hospital identified that only 42% of patients with thyroid cancer presenting with a thyroid nodule had preoperative fine-needle aspiration cytology (FNAC). In contrast, BAETS audit data from 2009 reported that 82% of treated patients, confirmed at histology to have a neoplastic lesion, underwent fine-needle aspiration (FNA) prior to the operation. The collection of such prospective information on endocrine surgical activity in the UK is crucial, not only for issues of surgical subspecialisation but for education and training. For UK surgeons, continuing full membership of the BAETS is conditional upon the submission of their clinical activity to the audit. It is likely in the future that General Medical Council (GMC) revalidation will require confirmation that surgeons take part in comparative national audit. The following standards and outcome measures are suggested as being applicable to current endocrine surgical practice.
Thyroid surgery
Standards
- •
The indications for operation, risks and complications should be discussed with patients prior to surgery.
- •
FNAC should be performed routinely in the investigation of solitary thyroid nodules.
- •
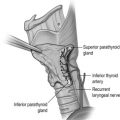
The recurrent laryngeal nerve should be routinely identified in patients undergoing thyroid surgery.
- •
All patients scheduled for re-operative thyroid surgery should undergo preoperative examination of their vocal cords by an ENT surgeon. All patients reporting voice change after thyroid surgery should undergo examination of their vocal cords. Permanent vocal cord palsy should not occur in more than 1% of patients.
- •
A return to theatre to control postoperative haemorrhage should occur in less than 5% of patients.
- •
All patients with thyroid cancer should be reviewed by the Cancer Centre designated specialist multidisciplinary team.
Outcome measures
There should be documented evidence to support that:
- •
The patient was informed of the indications for surgery and its risks and complications.
- •
FNAC was performed in at least 90% of patients prior to operation for solitary/dominant nodule.
- •
The recurrent laryngeal nerve(s) were identified during a surgical procedure.
- •
The permanent postoperative vocal cord palsy rate is not more than 1%.
- •
All patients scheduled for re-operative thyroid surgery have undergone preoperative examination of their vocal cords.
- •
The re-operation rate for postoperative haemorrhage after thyroidectomy is less than 5%.
- •
Patients with thyroid malignancy have been reviewed by the specialist multidisciplinary team.
Parathyroid surgery
Standards
In patients who undergo first-time operation for primary hyperparathyroidism:
- •
The indications for operation, risks and complications should be discussed with patients prior to surgery.
- •
The surgeon should identify and cure the cause of the disease in at least 95% of cases.
- •
All patients reporting voice change after parathyroid surgery should undergo examination of their vocal cords. Permanent vocal cord palsy should not occur in more than 1% of patients.
- •
All patients scheduled for re-operative parathyroid surgery should undergo preoperative examination of their vocal cords.
- •
Permanent hypocalcaemia should not occur in more than 5% of patients.
Outcome measures
There should be documented evidence to support that:
- •
The patient was informed of the indications for surgery and its risks and complications.
- •
After first-time parathyroid surgery, at least 90% of patients are normocalcaemic without calcium or vitamin D supplements.
- •
The permanent postoperative vocal cord palsy rate is not more than 1%.
- •
All patients scheduled for re-operative parathyroid surgery have undergone preoperative examination of their vocal cords.
Adrenal surgery
Standards
There should be multidisciplinary working to agreed diagnostic and therapeutic protocols to ensure that an appropriate strategy is developed for patients. This should include the management of the preoperative, perioperative and postoperative metabolic syndrome.
Outcome measures
There should be documented evidence to demonstrate that all patients have been discussed with the multidisciplinary team.
Biochemical cure should be evident in at least:
- •
95% of patients with phaeochromocytoma;
- •
95% of patients with Conn’s syndrome;
- •
95% of patients with Cushing’s syndrome.
Pancreatic surgery
Standards
- •
There should be multidisciplinary working to agreed diagnostic and therapeutic protocols to ensure that an appropriate strategy is developed for patients. This should include management of the preoperative, perioperative and postoperative metabolic syndrome.
- •
Patients with familial endocrine disease should be identified prior to surgery.
- •
The aims of any surgical procedure must be clearly defined prior to surgery.
Outcome measures
There should be documented evidence to demonstrate that all patients have been discussed with the multidisciplinary team:
- •
Insulinoma – surgery should result in biochemical cure in at least 90% of cases.
- •
Gastrinoma – surgery should result in biochemical cure or clinically useful response in at least 60% of cases.
Risk management
Risk management encapsulates the notion that all surgical activity involves some degree of risk and that the risk must be managed so as to achieve the best outcome for the patient. In the past it was sufficient merely to be properly trained, caring and conscientious; today, this does not suffice.
Medical care should be given effectively and carefully; in addition it must be seen to be given effectively and carefully. However cynical one might be about the mechanics of clinical governance and however self-confident one may feel as a professional, there is now a need to take public and documented steps to ensure that risk is being managed. There is evidence that the risk management process has positive advantages in terms of delivering a high quality of care, measured as an improved process of care with better outcome.
Staff issues
Are the consultants properly trained and up to date with their postgraduate education in endocrine surgery? Are consultants undertaking endocrine surgery on an occasional basis because they enjoy it rather than because they are trained in it? When appropriate, are complex patients referred to a specialist centre? The endocrine surgeon must be part of a team that includes endocrine physicians, oncologist, radiologists, cytopathologist and histopathologist, chemical pathologist and clinical/molecular geneticists.
Are trainees appropriately engaged in the process? Are surgical procedures delegated by an appropriate person in the full knowledge of the trainee’s competence? Is their supervision appropriate? It is not acceptable to let a new specialist trainee undertake a thyroidectomy prior to supervised assessment of their operative competence.
Communication issues
Are patients properly informed about proposed surgery, particularly the various therapeutic options open to them, in addition to the risks and implications of any choice they make (see ‘Consent’ below)? Are there information sheets available and in use?
Protocol issues
Are there written protocols in use to aid clinical decision-making, as well as local protocols for the care of patients with postoperative airway obstruction, hypocalcaemia and steroid replacement after adrenalectomy?
Record-keeping
Clear and contemporaneous evidence must be available in the notes, to show that patients were properly counselled prior to operation and warned about the risks of surgery. The operation notes should be contemporaneous, written by the operating surgeons (or at the very least countersigned by them) and should confirm that, for example, at thyroidectomy the recurrent laryngeal nerves were seen and protected and that parathyroid tissue was retained with its blood supply intact.
Support services
An increasingly common issue in litigation is delay in diagnosis or incorrect diagnosis. In this context it is imperative that the pathologists with whom you work should be competent in the specific and often difficult area of thyroid cytology and histology.
Audit
Remember that simply keeping audit records and having regular audit meetings is not sufficient. The audit cycle must be seen to be occurring such that what has been learned from audit is applied and the whole cycle repeated. Sadly this does not happen consistently.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


