Figure 15.1
39-year-old Caucasian male with a pink, ulcerated nodule on the right heel
Differential Diagnosis
Pyogenic granuloma
Basal cell carcinoma
Melanoma
Metastatic carcinoma
Angiosarcoma
Atypical fibroxanthoma
Spitz nevus
Adenocystic carcinoma
Squamous cell carcinoma
Biopsy Results
“Suggestive of adenocystic carcinoma.”
Diagnosis
Adenocystic carcinoma
Microscopic Feature
The classic findings of cutaneous adenocystic carcinoma (ACC) occur in the deep dermis and are characterized by basaloid cells in islands that form cribriform patterns and tubular structures (Fig. 15.2). Multiple cystic spaces can be seen containing mucin that stains positively with hyaluronic acid (Figs. 15.3 and 15.4). Perineural invasion is observed in most cases. The lumina of the tubular structures have prominent basement membrane material that is PAS positive and diastase-resistant [1–3].
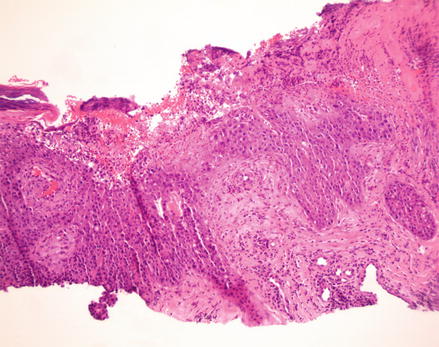
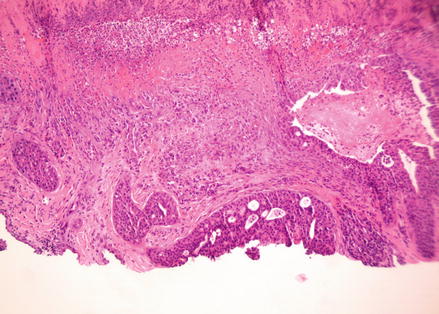
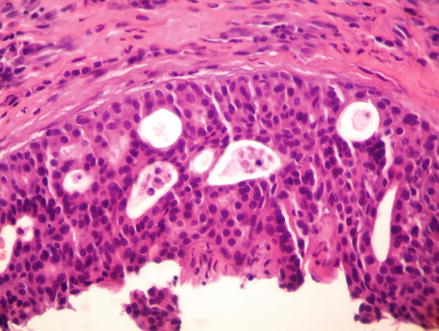
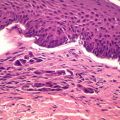
Figure. 15.2
H&E, 40×. Low magnification view shows an ulcerated epidermis with underlying nests of tumor
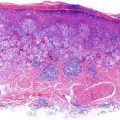
Figure 15.3
H&E, 40×. The tumor is invasive and extends into the deep dermis
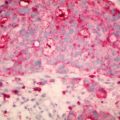
Figure 15.4
H&E, 400×. A close up of a basaloid nest which contains scattered round, cystic spaces (cookie cutter pattern)
Unlike the similarly appearing adenoid basal cell carcinoma, ACC typically does not have a connection to the overlying epidermis or adnexal structures. This separation is a helpful clue for pathologists when making the diagnosis, as oftentimes these two can be difficult to differentiate. Immunohistochemical studies demonstrate that cutaneous ACC stains positively for S-100, epithelial membrane antigen (EMA), and is occasionally positive for carcinoembryonic antigen (CEA) [1–3].
Related posts:
 Topical Treatment of Skin Cancers and the Risks of ‘Fighting Fire with Fire’
Topical Treatment of Skin Cancers and the Risks of ‘Fighting Fire with Fire’
 Amelanotic Malignant Melanoma of the Toe Presenting as an Ulcer: Management and Biopsy Guidelines
Amelanotic Malignant Melanoma of the Toe Presenting as an Ulcer: Management and Biopsy Guidelines
 Zosteriform Cutaneous Metastasis
Zosteriform Cutaneous Metastasis
 Metastatic Cutaneous Adenocarcinoma
Metastatic Cutaneous Adenocarcinoma
 Multiple Basal Cell Carcinomas and Superficial Radiotherapy (SRT)
Multiple Basal Cell Carcinomas and Superficial Radiotherapy (SRT)
 Balloon Cell Nevi and Balloon Cell Melanomas: What Are They?
Balloon Cell Nevi and Balloon Cell Melanomas: What Are They?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


