Table 90.1 Causes of unstable angina and non-ST-elevation myocardial infarctiona | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
to intense inflammation of the coronary arteries and result in complete coronary occlusion.22,23 Identification and treatment of these etiologies is dependent upon recognizing and treating the underlying diagnoses.
Table 90.2 Presentations of ACS | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
with each minute of delay associated with an increase in mortality.33 Reperfusion therapy to open the occluded artery with either fibrinolytics or primary PCI should be implemented urgently.
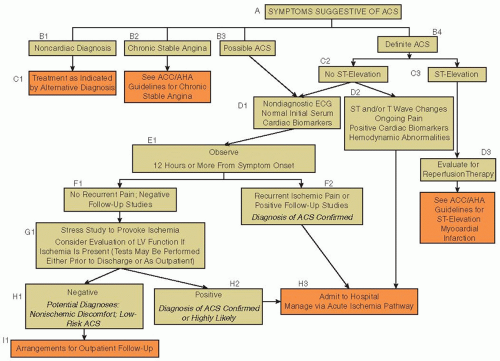 FIGURE 90.1 Treatment algorithm for patients with suspected ACS. ACC/AHA, American College of Cardiology/American Heart Association; ECG, electrocardiogram; LV, left ventricular. (From Anderson JL, Adams CD, Antman EM, et al., ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction. Circulation 2007;116(7):e148-e304.) |
for fibrinolytic therapy, the recommended door-to-needle time is ≤30 minutes. This means that from the minute the patient arrives in the emergency room to the minute the fibrinolytic infusion is begun, the time elapsed is not >30 minutes. For primary PCI, the established benchmark is a door-to-balloon time of ≤90 minutes.32
Table 90.3 Contraindications to fibrinolytic therapy in the management of STEMI | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||
medical therapy for NSTEMI and UA that includes antianginal, antiplatelet, and anticoagulant therapy (FIGURES 90.5 and 90.6).
Table 90.4 Cardiac biomarkers | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
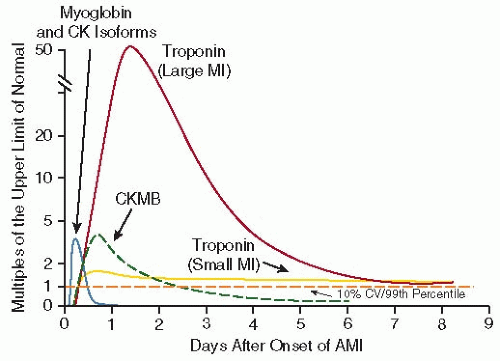 FIGURE 90.2 Release of biomarkers into the serum after acute myocardial infarction. The biomarkers are plotted showing the multiples of the cutoff for acute myocardial infarction (AMI) over time. The dashed horizontal line shows the upper limit of normal (ULN; defined as the 99th percentile from a normal reference population without myocardial necrosis; the coefficient of variation of the assay should be 10% or less). The earliest rising biomarkers are myoglobin and CK isoforms (leftmost curve). CK-MB (dashed curve) rises to a peak of 2 to 5 times the ULN and typically returns to the normal range within 2 to 3 days after AMI. The cardiacspecific troponins show small elevations above the ULN in small infarctions (e.g., as is often the case with NSTEMI) but rise to 20 to 50 times the ULN in the setting of large infarctions (e.g., as is typically the case in STEMI). The troponin levels may stay elevated above the ULN for 7 days or more after AMI. CK, creatine kinase; CKMB, MB fraction of creatine kinase; CV, coefficient of variation; MI, myocardial infarction. (Modified from Shapiro BP, Jaffe AS. Cardiac biomarkers. In: Murphy JG, Lloyd MA, eds. Mayo clinic cardiology: concise textbook, 3rd ed. Rochester, MN: Mayo Clinic Scientific Press and New York: Informa Healthcare USA, 2007:773-780. Used with permission of Mayo Foundation for Medical Education and Research. Also adapted from Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction). Circulation 2007;116(7):e148-e304.) |
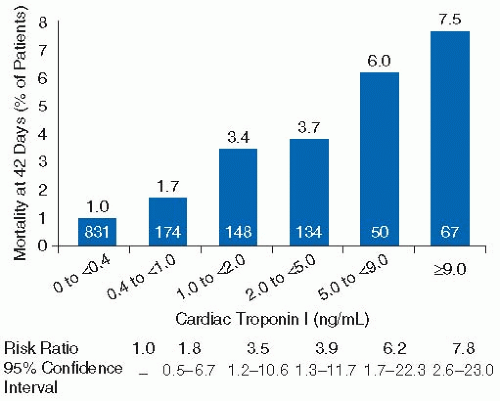 FIGURE 90.3 Stepwise association between elevations in troponin levels and death. (From Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction). Circulation 2007;116(7):e148-e304. Originally from Ohman EM, et al. Cardiac troponin T levels for risk stratification in acute myocardial ischemia. GUSTO IIA Investigators. N Engl J Med 1996;335(18): 1333-1341.) |
those with severe CAD who may benefit from revascularization.51,52 Furthermore, percutaneous revascularization of the culprit lesion may lead to a reduced risk for rehospitalization and reduced angina after discharge.53
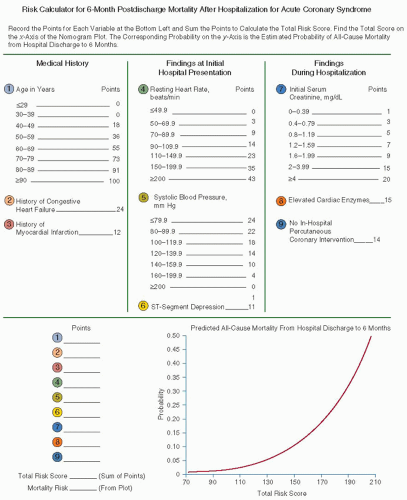 FIGURE 90.4 GRACE risk prediction model. (Adapted from Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction). Circulation 2007;116(7):e148-e304. Originally from Eagle KA, Lim MJ, Dabbous OH, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA 2004;291:2727-2733. Copyright © 2004 American Medical Association.) |
OR = 0.82; 95% CI, 0.72 to 0.93).54 This analysis showed an 18% relative reduction in death or MI, as well as a sustained reduction in mortality following discharge from the hospital with the invasive approach. In addition, the invasive strategy led to a reduction in angina, fewer hospitalizations, and improvements in quality of life.
Table 90.5 Thrombolysis in myocardial infarction risk scorea | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
Related posts:
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


