CLINICAL IMPLICATIONS
Part of “CHAPTER 10 – PINEAL GLAND“
SEXUAL MATURATION
The pineal gland and melatonin have been implicated in several clinical entities.5 Besides the possible link between gradually decreasing nocturnal melatonin levels and pubertal development (see Fig. 10-5), pineal tumors may alter sexual maturation (also see Chap. 92).20,21 Tumors of the pineal gland are more prevalent in men than in women and may either retard or advance sexual development.20 The opposite responses to space-occupying lesions of the pineal region are explained on the basis of cellular origin (i.e., parenchymal or nonparenchymal) and the consequential endocrine capabilities of the tumorous mass. In addition, these tumors can cause increased intracranial pressure and, because of associated hydrocephalic dilation of the third ventricle, Parinaud syndrome (paralysis of upward gaze and slightly dilated pupils that react normally on accommodation but not to light) (Fig. 10-6). Hypermelatoninism with an enlarged pineal gland has been shown to be associated with delayed sexual development.
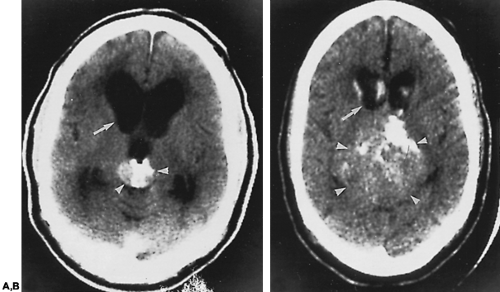 FIGURE 10-6. Computed tomographs (CTs) of a 67-year-old man with Parinaud syndrome and deteriorating mental status. Four years previously, the CT scan shown in A was obtained because of disorientation and dementia thought to be secondary to increased intracranial pressure. A 2-cm mass was seen in the pineal region (arrowheads) with triventricular dilation (arrow) (third and lateral ventricles). The fourth ventricle was not involved. The patient refused definitive surgery, and a ventriculoperitoneal shunt was performed. In the CT scan shown in B, the lesion has grown to 7 cm; the ventricles decreased in size considerably after shunt placement. (Courtesy of Dr. Frederick T. Borts.) |
OVULATORY RELATIONSHIPS
The observation that nocturnal melatonin levels may be lowest at the time of ovulation in women suggests that a decrease in the indoleamine concentration may permit ovulation.19 In animals, exogenously injected melatonin can inhibit both the release of ova and the surge of ovulatory hormones associated with this process. Melatonin may have a similar antiovulatory capability in humans when given in pharmacologic doses.22 Higher than normal nocturnal melatonin secretion is associated with hypothalamic amenorrhea in women, and with delayed puberty.23
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


