Chapter 68 Wilms’ Tumor
Wilms’ tumor, or nephroblastoma, is the most common childhood renal tumor, accounting for about 6% of pediatric malignant diseases.1 It was first described in 1814, but Max Wilms first identified the true nature of the condition as a neoplasm with mixed cellular elements in 1899.2,3 His name has become synonymous with nephroblastoma. The early advances in managing these small patients with huge tumors were made by surgeons, who reduced the operative mortality from 25% to the current rate of less than 1%. The survival of children with Wilms’ tumor gradually increased from less than 10% to about 50% by the 1940s and 1950s. Postoperative RT became routine after results from Boston Children’s Hospital documented an increased cure rate. The advent of effective chemotherapy (dactinomycin and vincristine) also had an impact on the survival of these children.4 The systematic development of multidisciplinary management for Wilms’ tumor resulted in a striking improvement in survival. Thus the grim outlook at the beginning of the 20th century (90% mortality rate) has effectively inversed to a survival rate of 90% in the early 21st century. Randomized clinical trials in North America under the aegis of the National Wilms’ Tumor Study Group (NWTS) and those in Europe, largely by the International Society of Pediatric Oncology (SIOP), have resulted in Wilms’ tumor therapy becoming a paradigm for successful multidisciplinary integration in the treatment of cancer. Successive NWTS clinical trials have been based on postoperative therapies, whereas preoperative strategies have been the focus of SIOP investigators.5,6
The clinical risk factors such as tumor stage and histology were categorized so that treatment could be modulated in intensity according to risk groups, the objective being to achieve cure with minimum complications. As a result, children with low-risk tumors now receive minimal therapy whereas those at high risk benefit from more intensive therapy. The modern survivors of Wilms’ tumor enjoy a better quality of life owing to sequential reductions in the intensity of therapy.7 Current Wilms’ tumor studies in the United States and Canada are conducted by the Children’s Oncology Group (COG).
Etiology and Epidemiology
The cause of Wilms’ tumor is unknown. The peak incidence is between 3 and 4 years of age. Wilms’ tumor may arise as sporadic or hereditary tumors or in the setting of specific genetic disorders.8 The overall annual incidence of Wilms’ tumor is 7.1 per million children, and approximately 500 new cases can be expected each year in North America. Wilms’ tumor is found more often in black than in white children, with a ratio of 1.25 : 1. Girls are affected more than boys in the same ratio.1
Prevention and Early Detection
Prevention awaits an identified cause. Uncommon congenital anomalies (aniridia, genitourinary malformations, hemihypertrophy, or signs of overgrowth) may be seen in 13% to 28% of children with unilateral or bilateral disease, respectively.9 Syndromes associated with a higher risk for developing Wilms’ tumor include the “WAGR” syndrome (aniridia, genitourinary malformation, mental retardation), the Beckwith-Wiedemann syndrome, and the Denys-Drash syndrome (see next section on molecular biology). Children with such syndromes should be screened for the development of Wilms’ tumor using ultrasonographic examinations of both kidneys every 3 months until age 5 years (WAGR) or 7 years (Beckwith-Wiedemann syndrome).8,10
Biologic Characteristics and Molecular Biology
The biologic characterization of Wilms’ tumor has provided the foundation for our understanding of key concepts in cancer genetics, including the roles of tumor suppressor genes and relation of genomic imprinting in tumorigenesis. Although Wilms’ tumor was one of the original examples in Knudson’s two-hit model of cancer development, subsequent research has shown that multiple genes and several genetic events contribute to the formation of this malignant disorder.11 The molecular changes that have been described in Wilms’ tumor can be classified as primary events predisposing to the development of tumor or secondary events associated with tumor progression.
WT1
Initial insights into the molecular biology of Wilms’ tumor were derived from the observation that in patients with WAGR syndrome the risk for developing the tumor is more than 30%. Cytogenetic analysis of individuals with this syndrome showed deletions at chromosome 11p13, which was later found to be the locus of a contiguous set of genes including PAX6, the gene causing aniridia, and WT1, one of the Wilms’ tumor genes. The WT1 gene encodes a transcription factor that is crucial to normal kidney and gonadal development.8 The Denys-Drash syndrome, which is characterized by pseudohermaphroditism, glomerulopathy, renal failure, and a 95% chance of Wilms’ tumor development, is caused by point mutations in the zinc-finger DNA-binding region of the WT1 gene.10 Although WT1 has a clear role in tumorigenesis of Wilms’ tumor in patients with the WAGR and Denys-Drash syndromes, only a minority of patients with sporadic Wilms’ tumor carries WT1 mutations in the germline (<5%) or in tumor tissue (6% to 18%).8
WT2
The Beckwith-Wiedemann syndrome is an overgrowth disorder manifested by large birth weight, macroglossia, organomegaly, hemihypertrophy, neonatal hypoglycemia, abdominal wall defects, ear abnormalities, and predisposition to Wilms’ tumor and other malignant disorders. Approximately 5% of individuals with this syndrome develop Wilms’ tumor. Beckwith-Wiedemann syndrome maps to chromosome 11p15, a locus called WT2 because loss of heterozygosity (LOH) at this locus has been detected in Wilms’ tumor.12
The WT2 locus consists of several genetically imprinted genes that are in two clusters or imprinting centers. Several combinations of genetic and epigenetic alterations can give rise to Beckwith-Wiedemann syndrome, with increasing recognition of genotype-phenotype relationships.13,14 Imprinting Center 1, which contains the IGF2 and H19 genes, has been most implicated in Wilms’ tumor predisposition. Alterations in Imprinting Center 2, which contains the genes CDKN1C, KCNQ1 and KCNQ1OT1, are not strongly linked to Wilms’ tumor development.
Familial Wilms’ Tumor Genes
Familial predisposition to Wilms’ tumor is rare, identified in only 1.5% of patients. A few families were shown to carry constitutional mutations of the WT1 gene, but genetic linkage analysis has excluded WT1 in most familial Wilms’ tumor pedigrees. Linkage analysis has uncovered two familial Wilms’ tumor loci, FWT1 (17q) and FWT2 (19q), but the causative genes remain to be identified.8
Wnt Signaling Pathway Genes (WTX and β-Catenin)
Alterations of the Wnt signaling pathway have been implicated in several human malignancies. Central to the pathway is the activator, β-catenin, which is degraded in the absence of Wnt signaling. Activating mutations in the gene encoding β-catenin (CTNNB1) occur in approximately 15% of Wilms’ tumors.15 Interestingly, mutations in CTNNB1 occur mostly in tumors in which WT1 is also mutated, suggesting that these two events cooperate in the formation of Wilms tumor. WTX, a recently discovered novel Wilms tumor suppressor gene on the X chromosome, is inactivated in one third of sporadic Wilms’ tumor cases. In contrast to the “two-hit” model of inactivation of WT1, WTX is inactivated by a monoallelic “single hit” event that targets the X chromosome in tumors in males and the active X chromosome in tumors in females.16 WTX has been shown to be a negative regulator of Wnt/β-catenin signaling.17
Loss of Heterozygosity at 1p and 16q
One of the major goals of the NWTS-5 trial was to prospectively analyze the prognostic significance of LOH at chromosomes 1p and 16q. Analysis of these data revealed that the relative risks for relapse for patients with stage I to IV favorable histology tumors with LOH stratified by stage are 1.77 for LOH 1p (p <.01) and 1.39 for LOH 16q (p = .05). When the effects of LOH for both 1p and 16q were considered jointly, the relative risk for relapse in stage I and II favorable histology disease was 2.88 (p = .001) and that for stage III and IV favorable histology disease was 2.41 (p = .01). The relative risk for death for patients with stage I and II favorable histology disease with LOH for both regions is 4.25 (p = .01), and for stage III and IV it is 2.66 (p = .04).18
Pathology and Pathways of Spread
Most Wilms’ tumors are solitary lesions, although 6% involve both kidneys and 12% show multifocal involvement within a single kidney. The classic triphasic “favorable histology” Wilms’ tumor consists of varying proportions of three cell types—blastemal, stromal, and epithelial—recapitulating various stages of normal renal development (Fig. 68-1A, B). Less commonly, heterologous epithelial or stromal components are identified, including mucinous or squamous epithelium, skeletal muscle, cartilage, osteoid, or fat. Not all specimens are triphasic; biphasic and monophasic patterns are frequently encountered. Favorable histologic features characterize 87% of Wilms’ tumors.19,20
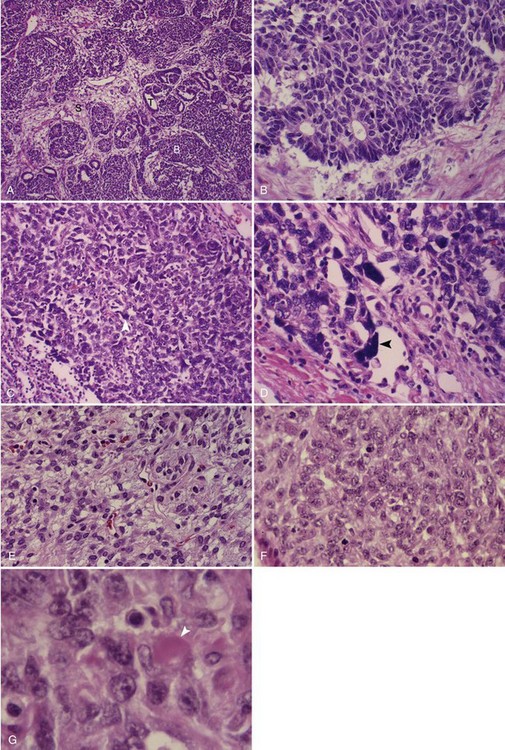
The histologic feature of greatest clinical significance is anaplasia, defined by the presence of greatly enlarged polyploid nuclei (see Fig. 68-1C, D). Anaplasia is present in approximately 8%; it is rare in the first 2 years of life and increases in frequency to approximately 13% in children older than age 5 years. Anaplasia is far more frequent in African-American than in white patients and has been strongly linked to the presence of TP53 mutations.21,22 The distinction between focal and diffuse anaplasia is prognostically significant.23
Correlations between histologic characteristics and clinical behavior have identified blastemal-rich tumors as typically invasive, presenting at an advanced stage, if often responsive to chemotherapy. By contrast, predominantly epithelial and rhabdomyomatous Wilms’ tumors are more likely to present at a low stage, yet many are relatively chemotherapy resistant. Analysis of the cohort of young children with small stage I intrarenal tumors assigned no adjuvant chemotherapy provides further support for the excellent prognosis of epithelial-differentiated Wilms’ tumors.24 Although much of the past success of the NWTS has relied on accurate histologic subclassification of Wilms’ tumors to define high-risk and low-risk subtypes, further risk classification is likely to depend on molecular genetic features.
The existence of precursor lesions (nephrogenic rests) is rather common. These lesions consist of abnormally persistent intrarenal embryonal nephroblastic tissue with small clusters of blastemal cells, tubules, or stromal cells. Nephrogenic rests can be subclassified by their positions within the kidney and histologic appearance: perilobar nephrogenic rests are limited to the periphery of the renal cortex, and intralobar nephrogenic rests occur randomly throughout the renal lobe. Nephroblastomatosis refers to the presence of multiple nephrogenic rests typically throughout the kidney. There are several possible fates for nephrogenic rests: most become dormant or involute spontaneously; only a small number develop clonal transformation into Wilms’ tumor. The presence of nephrogenic rests within a kidney resected for Wilms’ tumor indicates the need for monitoring the contralateral kidney for tumor development, particularly in young infants.25
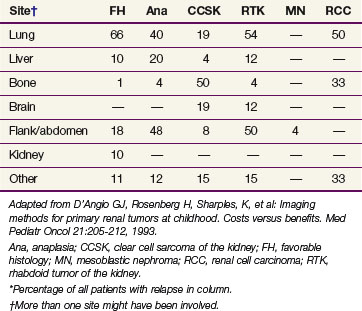
The other major cellular types of kidney tumors are outlined in Table 68-1, including:
Clinical Manifestations, Patient Evaluations, and Staging
Laboratory evaluation after physical examination should include a complete blood cell count, routine hepatic and renal chemistries, and urinalysis, noting the presence or absence of urinary protein and white or red blood cells. Imaging studies before surgery are designed to evaluate the extent of the renal mass and differentiate primary intrarenal tumors from neuroblastoma (most often arising from the adjacent suprarenal gland or retroperitoneal structures), the presence of a normally functioning, morphologically normal contralateral kidney, the presence of a patent renal vein and inferior vena cava (i.e., free from thrombosis, most often tumor thrombosis when seen), and the presence or absence of metastases in the lungs. Diagnostic imaging studies include abdominal ultrasonography (particularly useful in the detection of tumor thrombosis) and CT or MRI of the abdomen (Fig. 68-2). A chest radiograph or CT scan of the chest can be used to detect lung metastasis. The clinical significance of metastatic tumors detected by chest CT but not on chest radiographs remains unclear, although evidence is increasing that some of these patients do not fare well with chemotherapy with vincristine and dactinomycin alone.28,29 MRI of the abdomen can help to distinguish between nephrogenic rests and Wilms’ tumor.30 Postoperatively, when the histology is established, a bone scintiscan and skeletal survey should be obtained for patients with CCSK, RTK, and RCC and MRI of the brain should be performed for those with RTK and RCC.

Staging
Wilms’ tumors are staged on the basis of anatomic tumor extent; therapy is currently based on stage and histology.31 Classifications based on tumor extent have evolved over the years. After analysis of the prognostic significance of several clinicopathologic factors in NWTS-1 and NWTS-2, an NWTS staging system has been in use from NWTS-3 onward. Patients with lymph node involvement, previously included with stage II disease, are now classified as having stage III disease, and those with local tumor spill were moved from stage III to stage II disease.32 Refinements to the inclusion criteria for stages I and II disease were introduced in the NWTS-5 study. Criteria for stage I were refined to accommodate an important subset of Wilms’ tumor currently managed by nephrectomy alone. Before NWTS-5, the distinction between stages I and II in the renal sinus was established by the hilar plane, which was an imaginary plane connecting the most medial aspects of the upper and lower poles of the kidney. This criterion was difficult to apply because of tumor distortion, and thus the hilar plane criterion has been replaced with renal sinus vascular or lymphatic invasion. The latter definition includes not only the involvement of vessels within the hilar soft tissue but also vessels located in the radial extensions of the renal sinus into the renal parenchyma.33,34
The current COG staging guidelines for Wilms tumor are shown in Table 68-2. These guidelines are essentially similar to those for NWTS-5 except for the fact that children with tumor spillage are upstaged from stage II to stage III because of the higher risk for relapse in these patients with two-drug chemotherapy absent use of RT.35
TABLE 68-2 Children’s Oncology Group Staging of Wilms’ Tumor (2010)
| Stage | Description |
|---|---|
| I |