will then accumulate in the liver, specifically in the microsomes.17 Warfarin is a racemic mixture of S and R enantiomers, which are present in almost equal proportions. Warfarin has a half-life of 36 to 42 hours, which is the result of different metabolism rates of the two enantiomers. The R enantiomer is less potent, is metabolized primarily by two microsomal cytochrome enzymes (CYP1A2 and CYP3A4) to 6- and 8-hydroxywarfarin, and has a half-life of 45 hours. The S enantiomer is 2.7 to 3.8 times more potent than the R enantiomer, is metabolized primarily by the CYP2C9 enzyme of the P450 system to 7-hydroxywarfarin, and has a half-life of 29 hours (FIGURE 106.1B).18 The inactive hydroxywarfarins are excreted renally.
 FIGURE 106.1 A,B: Metabolism of vitamin K and warfarin. (From HirshJ, Dalen J, Guyatt G. The sixth [2000] ACCP guidelines for antithrombotic therapy for prevention and treatment of thrombosis. American College of Chest Physicians. Chest 2001;119:1S-2S; Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133:160S-198S.) |
Table 106.1 Level of evidence for drug, food, and dietary supplement interactions with warfarin | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 106.2 Distribution of CYP2C9 and VKOR polymorphisms in different racial populations* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
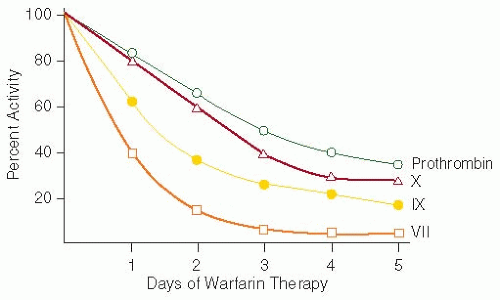 FIGURE 106.2 Effects of warfarin therapy on the plasma vitamin K-dependent procoagulant proteins. Administration of 5 to 10 mg daily of warfarin results in inhibition of synthesis of functional vitamin K-dependent proteins. The coagulant activity of these proteins in plasma declines as a function of their half-life. Half-lives of factors VII, IX, and X and prothrombin are 6,24, and 40 and 60 hours, respectively. Although 1 to 2 days of warfarin prolongs the PT assay (because of the rapid decrease in factor VII concentration), therapeutic anticoagulation requires at least 4 to 5 days. (Data from O’Reilly RA.The pharmacodynamics of the oral anticoagulant drugs. Prog Hemost Thromb 1974;2:175-213; reproduced from Greenberg PL, Negrin R, Rodgers GM. Hematologic disorders. In: Melmon KL, Morrelli HF, Hoffman BB, et al., eds. Clinical pharmacology: basic principles in therapeutics, 3rd ed. New York: McGraw-Hill, 1992:524-599, with permission; from Wintrobe MM, Greer JP. Wintrobe’s clinical hematology, 12th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2009:1488, Ref. 178.) |
(FIGURE 106.3).64 With the wide use of the standardized INR, several of its limitations have become apparent (Table 106.3). These include decreased precision when insensitive thromboplastins are used; there is an incorrect assignment of an ISI value by the manufacturer; a different reagent-instrument combination is used than that recommended by the manufacturer; and if an incorrect control PT value is used.45
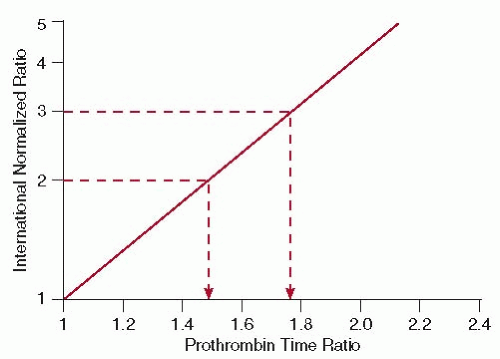 FIGURE 106.3 Relationship between PT ratio on warfarin therapy and the corresponding INR. The slope of the line represents the ISI value of the particular thromboplastin preparation used in the laboratory’s PT assay. In this example, for low-intensity warfarin therapy (INR 2.0 to 3.0), a PT ratio between 1.50 and 1.75 would be required. Thromboplastins with higher ISI values would have slopes greater than that shown and would be less sensitive reagents for the PT assay, whereas thromboplastins with lower ISI values would have slopes less than that shown (more sensitive reagents). (From Greenberg PL, Negrin R, Rodgers GM. Hematologic disorders. In: Melmon KL, Morrelli HF, Hoffman BB, et al., eds. Clinical pharmacology: basic prìinciples in therapeutics, 3rd ed. New York: McGraw-Hill, 1992:524-599, with permission; from Wintrobe MM, Greer JP. Wintrobe’sclinical hematology, 12th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2009:1490.) |
Related posts:
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Unusual Sites of Arterial Occlusion
Unusual Sites of Arterial Occlusion
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


