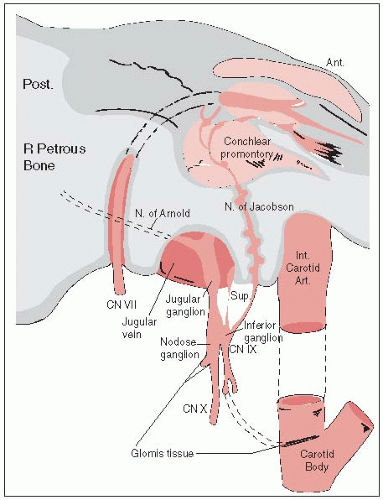
Glomus bodies are found in the jugular bulb and along the tympanic (Jacobson) and auricular (Arnold) branch of the tenth nerve in the middle ear or in other sites (Fig. 20-1).
Glomus tumors (chemodectoma or paraganglioma) can be classified as tympanic (middle ear), jugulare, or carotid vagal, or may originate from other locations such as the larynx, adventitia of thoracic aorta, abdominal aorta, or surface of the lungs.
Although histologically benign, they may extend along the lumen of the vein to regional lymph nodes, but rarely to distant sites.
Clinical Presentation
Glomus tumors of the middle ear may initially cause earache or discomfort, pulsatile tinnitus, or hearing loss; in later stages, cranial nerve paralysis results from invasion of the base of skull (10% to 15%) (43).
If the tumor invades the middle cranial fossa, symptoms may include temporoparietal headache, retro-orbital pain, proptosis, and paresis of cranial nerves V and VI. If the posterior fossa is involved, symptoms may include occipital headache, ataxia, and paresis of cranial nerves V to VII, IX, and XII; invasion of the jugular foramen causes paralysis of nerves IX to XI.
Chemodectoma of the carotid body usually presents as a painless, slowly growing mass in the upper neck; occasionally, it may be pulsatile and have a thrill or bruit. As it enlarges, it may extend into the parapharyngeal space and be visible on examination of the oropharynx (40).
Diagnostic evaluation for glomus tumors of the ear and base of skull is outlined in Table 20-1.
High-resolution computed tomography (CT) with contrast has the highest degree of sensitivity and specificity.
Biopsy of glomus tumors may result in severe hemorrhage.
FIGURE 20-1 Anatomy of the region of the glomus jugulare. (From Hatfield PM, James AE, Schulz MN. Chemodectomas of the glomus jugulare. Cancer 1972;30:1165-1168, with permission.)
Staging
Prognosis is closely related to anatomic location and volume of lesion, as reflected in the Glasscock-Jackson classification. An alternative classification was proposed by McCabe and Fletcher (38) (Table 20-2).
General Management
Surgery
Surgery generally is used to treat small tumors that can be completely excised.
Percutaneous embolization of a low-viscosity silicone polymer has been used, frequently as preoperative preparation of the tumor.
Surgical treatment of a glomus tumor arising in the jugular bulb requires more complex surgical approaches involving the base of the skull. It often consists of piece-by-piece removal, which is accompanied by significant bleeding and damage to adjacent neurovascular structures.
Radiation Therapy
Irradiation frequently is used to treat glomus tumors, particularly those in the tympanicum and jugulare bulb (52), or carotid body chemodectomas (40).
Tumors with destruction of petrous bone, jugular fossa, or occipital bone are more reliably managed with irradiation, as are patients with jugular foramen syndrome (45).
Some reports describe successful combinations of surgery with either preoperative or postoperative irradiation (41, 52).
TABLE 20-1 Diagnostic Workup for Glomus Tumors of The Ear and Base of Skull, Hemangiopericytoma, Esthesioneuroblastoma, Extramedullary Plasmacytoma, and Sarcoma of the Head and Neck
General
History
Physical examination
Radiographic Studies
CT scan to define tumor extent and possible central nervous system involvement
Plain radiographs, including temporal bone views
MRI with gadolinium
Arteriography to determine bilateral involvement and collateral cerebral blood flow (optional)
Jugular phleborheography (optional)
Laboratory Studies
Complete blood counts on admission
Blood chemistries
Urinalysis
Special Tests
Audiograms to establish baseline hearing loss
Histologic staining to determine presence of catecholamines
TABLE 20-2 Modification of McCabe and Fletcher Classification of Chemodectomas
Tumor group
Characteristics
Group I
Tympanic tumors
Absence of bone destruction on x-rays of the mastoid bone and jugular fossa; absence of facial nerve weakness; intact eighth nerve with conductive deafness only; intact jugular foramen cranial nerves (IX, X, and XI)
Group II
Tympanomastoid tumors
X-ray evidence of bone destruction confined to mastoid bone and not involving petrous bone; normal or paretic seventh nerve; intact jugular foramen nerves; no evidence of involvement of superior bulb of jugular vein on retrograde venogram
Group III
Petrosal and extrapet-rosal tumors
Destruction of the petrous bone, jugular fossa, and/or occipital bone; positive findings on retrograde jugulography; destruction of petrous or occipital bones on carotid arteriogram; jugular foramen syndrome (paresis of cranial nerves IX, X, or XI); or presence of metastasis
Source: From Wang M-L, Hussey DH, Doornbos JF, et al. Chemodectoma of the temporal bone: a comparison of surgical and radiotherapeutic results. Int J Radiat Oncol Biol Phys 1988;14:643-648.
Radiation Therapy Techniques
Limited (usually unilateral) portals should be used for relatively localized glomus tumors, regardless of whether the treatment is combined with surgery.
Dickens et al. (14) used a three-field arrangement with a superior-inferior wedged and lateral open field, with a weighting of 1.00 to 1.00 to 0.33.
Electrons (15 to 18 MeV) with a lateral portal or combined with 60Co or 4- to 6-MV photons (20% to 25% of total tumor dose) render a good dose distribution.
For tumor that has spread into the posterior fossa, parallel-opposed portals with 6- to 18-MV photons may be needed.
Dose is 45 to 55 Gy in 5 weeks in 1.8- to 2.0-Gy daily fractions, five treatments per week (10).
Stereotactic radiosurgery has shown promise in local control of this tumor. The median dose using gamma knife radiosurgery is 15 Gy. PFS is close to 100% at 5 years and 75% at 10 years (44)
HEMANGIOPERICYTOMA
Hemangiopericytoma is an unusual vascular tumor; although it may occur anywhere in the body, the head and neck are the most common locations after the lower extremities and retroperitoneum.
Clinical Presentation
In the head and neck, hemangiopericytoma may be a polypoid, painless, soft gray or red mass that grows slowly and may cause nasal obstruction; epistaxis is common.
On arteriography, hemangiopericytoma is the only vascular tumor that has characteristic angiographic features, including radially arranged or spider-like branching vessels around and inside the tumor and a long-standing, well-demarcated tumor stain.
General Management
Complete local resection, if possible, combined with preoperative embolization of tumor, is the treatment of choice.
More extensive surgery is required for tumors with malignant features.
For incompletely resected tumors, postoperative irradiation is used (36).
The role of chemotherapy is not well determined.
Radiation Therapy Techniques
Use of radiation therapy alone is controversial.
The main role of irradiation is either as an adjuvant after complete excision of the lesion or postoperatively for minimal residual disease (30).
Tumor doses of 60 to 65 Gy in 6 to 7 weeks are required to produce local tumor control in postoperative cases (29).
The tumor is considered relatively radioresistant; an effective dose for hemangiopericytoma is 75 to 90 Gy in 30 to 60 days (22).
Irradiation fields should be wide and encompass the tumor bed with a safe margin of at least 5 cm to avoid marginal recurrence.
Portal arrangement and beam selection are similar to those used to treat malignant brain tumors or soft-tissue sarcomas.
CHORDOMAS
Anatomy
Chordomas are rare neoplasms of the axial skeleton that arise from the remnants of the primitive notochord (chorda dorsalis).
Basisphenoidal chordoma may be difficult to differentiate histologically from chondroma and chondrosarcoma, and radiographically from craniopharyngioma, pineal tumor, and hypophyseal and pontine glioma.
Natural History
Lethality rests on critical location, aggressive local behavior, and extremely high local recurrence rate.
Lymphatic spread is uncommon.
The incidence of metastasis, which is reported to be as high as 25%, is greater than previously believed and may be related to the long clinical history. The most common site of distant metastasis is the lung, followed by liver and bone (43).
Prognostic Factors
Aside from histology, prognostic factors that most influence choice of treatment are location, local extent of tumor, and surgical resectability.
Clinical Presentation
In the head, extension may be intracranial or extracranial, into the sphenoid sinus, nasopharynx, clivus, and sellar and parasellar areas, with a resultant mass effect.
In the spheno-occipital region, the most common presenting symptom is headache.
Other presentations include symptoms of pituitary insufficiency, nasal stuffiness, bitemporal hemianopsia, diplopia, and other cranial nerve deficits.
Cranial nerve palsies are common in patients with clivus chordoma.
Diagnostic Workup
Diagnostic workup varies with primary location of disease.
Most patients have significant bony destruction; some have calcifications in the tumor. Plain x-ray films and CT scans are highly useful; contrast enhancement is required.
Magnetic resonance imaging (MRI) is inferior to CT in its ability to demonstrate bony destruction and intratumoral calcification but is superior to CT in delineation of exact tumor extent.
Because of its greater availability and lower cost, CT is the technique of choice for routine follow-up of previously treated patients.
General Management
A surgical approach is preferentially recommended (when feasible), but complete surgical extirpation alone is unusual.
Because of surgical inaccessibility, relative resistance to irradiation, and a high incidence of local recurrence, combined surgical excision and irradiation is frequently used.
Radiation Therapy Techniques
Irradiation techniques vary considerably, depending on location of tumor.
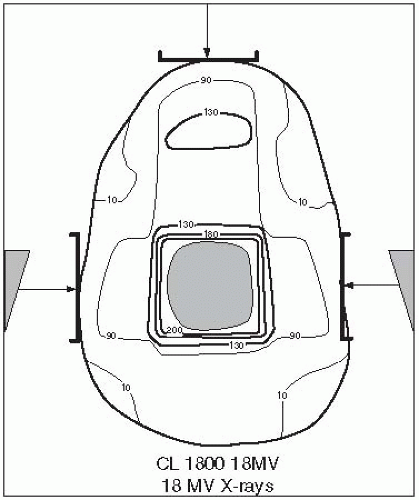
Basisphenoidal tumors are usually treated by a combination of parallel-opposed lateral fields, anterior wedges, and photon and electron beam combinations, depending on extent of tumor (Fig. 20-2).
FIGURE 20-2 Treatment planning field arrangement for clivus chordoma. (From Perez CA, Chao KSC. Unusual nonepithelial tumors of the head and neck. In: Perez CA, Brady LW, eds. Principles and practice of radiation oncology, 3rd ed. Philadelphia, PA: Lippincott-Raven, 1998:1095-1134, with permission.)
Precision radiation therapy planning, preferably using CT and MRI when available, is required.
Portal margins are 1 to 2 cm around the tumor.
Frequently used doses are 55 to 66 Gy (median, 60 Gy) in 1.8- to 2.0-Gy fractions (23).
Stereotactic irradiation has been used in some patients (32).
Because of the slow proliferative nature of chordomas, high linear energy transfer may be useful. Proton beam boosts have been recommended (19).
Brachytherapy can be used for recurrent tumors of the base of skull or adjacent to the spine when more aggressive surgical exposure is offered (24).
Sequelae of Treatment
In patients treated with high irradiation doses or charged particles, sequelae include brain damage, spinal cord injury, bone or soft-tissue necrosis, and xerostomia (43).
Some patients experience unilateral vision loss or radiation injury to the brainstem (5).
After high-dose proton therapy for clivus tumors, the actuarial incidence of endocrine abnormalities was 26% at 3 years and 37% at 5 years; hypothyroidism was the most frequent abnormality (49). The dose to the pituitary in patients with abnormalities was equivalent to 63.1 to 67.7 Gy.
LETHAL MIDLINE GRANULOMA
Lethal midline granuloma (LMG, midline malignant polymorphic reticulosis [PMR]) is characterized by progressive, unrelenting ulceration and necrosis of the midline facial tissues. It is associated with Epstein-Barr virus.
Considerable controversy exists regarding disorders characterized by a necrotizing and granulomatous inflammation of the tissues of the upper respiratory tract and oral cavity (43). If other etiologies can be excluded, three clinicopathologic entities remain:
Wegener’s granulomatosis is an epithelioid necrotizing granulomatosis with vasculitis of small vessels. Systemic involvement of the kidneys and lungs is common.
Polymorphic reticulosis is an unusual disorder characterized by atypical, mixed lymphoid infiltration of the submucosa with extensive areas of necrosis, sometimes extending to bone or cartilage. Most (if not all) cases of PMR are peripheral T-cell lymphomas.
Idiopathic LMG is a localized disorder characterized by destruction of the midfacial area; if left untreated, it is uniformly fatal.
Despite specific clinicopathologic features, the distinction between LMG and PMR is often difficult to make. In fact, these disorders may represent two phases of the same disease, with LMG remaining histologically benign or evolving into PMR, although this is controversial.
Most patients have involvement of the nasal cavity (including destruction of septum) and paranasal sinuses (particularly maxillary antrum).
The primary lesion may extend into the orbits, oral cavity (palate, gingiva), or even the pharynx.
Clinical Features and Diagnostic Workup
Clinical manifestations include progressive nasal discharge, obstruction, foul odor emanating from the nose, and, in later stages, pain in the nasal cavity, paranasal areas, and even in the orbits.
Examination discloses ulceration and necrosis in the nasal cavity, perforation or destruction of nasal septum and turbinates, and even ulceration of the nose.
Edema of the face and eyelids may be noted; the bridge of the nose may be sunken.
Radiographic studies initially show soft-tissue swelling, mucosal thickening, and findings consistent with chronic sinusitis.
CT is invaluable in demonstrating the full extent of the tumor, including bone or cartilage destruction.
General Management and Radiation Therapy Techniques
When treatment is planned, it is extremely important to exclude the diagnosis of Wegener’s granulomatosis, a benign process that is commonly treated with steroids and systemic chemotherapy. Bona fide LMG does not respond to steroids, and the treatment of choice is radiation therapy (48).
Target volume should encompass all areas of involvement, including adjacent areas at risk (i.e., for a lesion of the maxillary antrum it would include the antrum and all of the paranasal sinuses), with a 2- to 3-cm margin (25). Wide margins are necessary because marginal failures are a significant problem (50).
Irradiation techniques are similar to those for tumors of the paranasal sinuses, nasal cavity, or nasopharynx (43).
Only gold members can continue reading. Log In or Register to continue