Adrenal “incidentaloma” is frequently ignored by clinicians. However, approximately 50% of all patients with adrenocortical carcinomas (ACCs), pheochromocytomas, and overt hormone excess are discovered incidentally. When imaging characteristics of the adrenal mass do not clearly exclude malignancy (i.e., malignancy is excluded if the unenhanced computed tomography [CT] attenuation is <10 Hounsfield units [HU]), , further action is needed, and may include imaging monitoring, another imaging test, or adrenalectomy. Urine steroid profiling was recently validated as an accurate diagnostic test for ACC.
Case Report
The patient was a 21-year-old woman who 7 months prior presented to a local emergency department with symptoms of abdominal pain. CT of the abdomen demonstrated appendicitis, and she was treated with appendectomy. She recovered well, but on review of her hospital records noticed that the CT report also mentioned a 2.7 × 2.1 cm left adrenal mass. This discovery prompted her to perform internet research on adrenal tumors, and on reviewing the symptoms of Cushing syndrome, she requested her primary care physician to perform a hormonal workup and repeat the CT scan. Her symptoms included weight gain of 10 pounds over 3 months (unusual for her), exacerbation of anxiety and depression, and fatigue. She was a dancer, and despite intensifying her training, she noticed muscle weakness. In addition, she observed easy bruising and development of striae over her abdomen. On physical examination her body mass index was 24.1 kg/m 2 and blood pressure was 110/80 mmHg. She presented clear cushingoid features, including facial rounding, dorsocervical and supraclavicular pads, facial plethora, and a few small striae.
INVESTIGATIONS
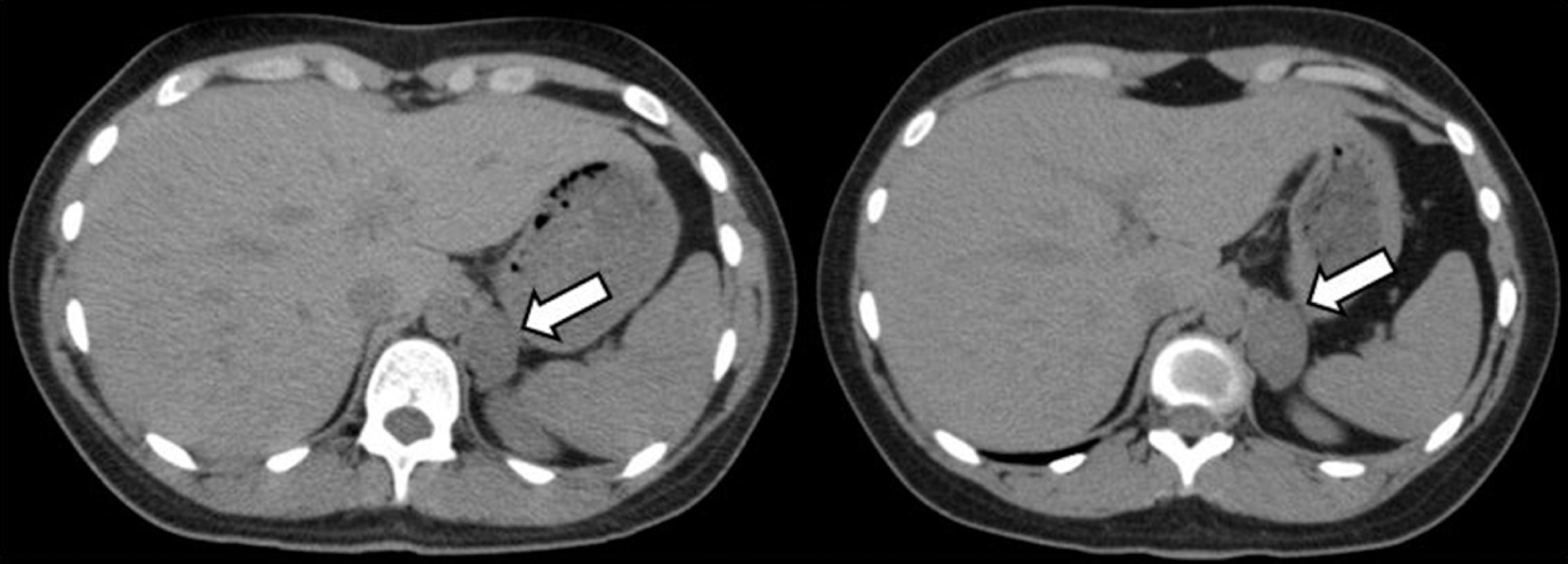
The patient’s self-diagnosis of Cushing syndrome related to her adrenal mass (corticotropin [ACTH]-independent hypercortisolism) was completely accurate ( Table 24.1 ). Both the abdominal CT scan obtained at the time of appendicitis (7 months prior) and the scan performed several weeks before referral were reviewed. On the contrast-enhanced CT scan from 7 months prior, a 2.2 × 2.9 × 2.7–cm left adrenal mass was demonstrated. Follow-up CT scan demonstrated an enlargement of the adrenal mass, measuring 2.5 × 3.6 × 3.2 cm; it had an unenhanced CT attenuation of 27 Hounsfield units (HU) and an absolute contrast washout of 74% at 10 minutes after contrast administration ( Fig. 24.1 ). In addition, the patient provided a 24-hour urine sample for steroid profiling analysis: a research procedure at that time but now clinically available ( http://www.mayocliniclabs.com/test-catalog/Overview/604986 ) ( Table 24.2 ).
| Biochemical Test | Result | Reference Range |
| am cortisol, mcg/dL | 9.2 | 7–25 |
| pm cortisol, mcg/dL | 8.7 | 2–14 |
| Post–1-mg DST cortisol, mcg/dL | 16 | <1.8 |
| ACTH, pg/mL | <5 | 10–60 |
| DHEA-S, mcg/dL | 77 | 44–332 |
| 24-Hour urine metanephrine, mcg/dL | 52 | 30–180 |
| 24-Hour urine normetanephrines, mcg/dL | 134 | 103–390 |
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


