Tumors of the Heart, Pericardium, and Great Vessels
 ANATOMY
ANATOMY
The heart is a hollow, conical [MB1]organ with muscular walls. In the adult, it measures approximately 12 cm in length, 8 to 9 cm in width, and 6 cm in thickness. It is located in the inferior aspect of the middle mediastinum, with two-thirds lying to the left of midline and one-third to the right. The heart lies posterior to the sternum and rib cage, and anatomic landmarks on the chest wall may be used to approximate its position. The apex is located roughly 8 cm to the left of midline in the fifth intercostal space, and the base is at the level of the third costal cartilage. It rests on the diaphragm inferiorly. The heart receives its blood supply from the coronary arteries, which are located in the space between the myocardium and epicardium. The pericardial fat provides a smooth contour and is also located in this space. The heart has four chambers: two ventricles with thick muscular walls and two atria with thin muscular walls. Although the heart is not attached to surrounding organs, it is held in position by its association with the great vessels (GV) and the pericardium. The GV include the aorta, superior and inferior venae cava (IVC), pulmonary artery, and pulmonary veins, which arise from (or terminate in) the left ventricle, right atrium, right ventricle, and left atrium, respectively. The roots of the GV, along with the heart, are encompassed by the parietal pericardium. In combination with the epicardium, this fibrous layer provides a smooth cavity in which the heart can pump freely. Externally the pericardium is adherent to, but separate from, the mediastinal pleura, creating a potential space through which the phrenic nerve traverses.1
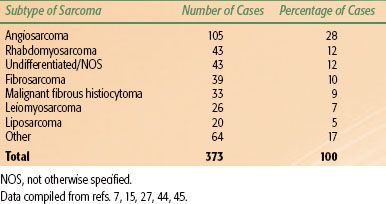
TABLE 54.1 DISTRIBUTION OF HISTOLOGIC SUBTYPES OF CARDIAC SARCOMA
 INCIDENCE AND EPIDEMIOLOGY
INCIDENCE AND EPIDEMIOLOGY
Tumors of the heart, GV, and pericardium are rare and include a range of disease presentations: primary neoplasms; secondary metastases from a known malignancy; or direct tumor invasion into the structures, which is seen in certain cancers such as Hodgkin or non-Hodgkin lymphoma, lung cancer, or malignant thymoma. The focus of this chapter will be to review the epidemiology, diagnosis, natural history, and management of primary tumors arising from the heart, pericardium, and GV, as well as metastatic disease to these sites.
The first described case of a primary cardiac tumor was by Albers in 1835.2 Reynen3 performed a compilation of autopsy series consisting of over 700,000 cases and found 157 primary cardiac tumors. The overall incidence of primary tumors is 0.021%, with a range from 0% to 0.19%. Approximately 75% of primary tumors of the heart are benign, and about half of those are atrial myxomas arising from the interatrial septum.4–6 Lipomas, papillary fibroelastomas, and rhabdomyomas each account for approximately 10% of cases. Fibromas, hemangiomas, and teratomas are less common benign cardiac tumors.7 Cystic atrioventricular node tumors are extremely rare but may lead to sudden death, despite their small size.8 There is an increased incidence of cardiac myxomas among females and in patients with Carney complex, an inherited autosomal dominant disorder that also shows hyperpigmented lentigines, blue nevi, schwannomas, endocrine tumors, and endocrinopathies.9,10 The syndrome is most commonly caused by an inactivating germline mutation of the PRKAR1 A tumor-suppressor gene on chromosome 17q23-q24.9,11,12 Variants include the LAMB (lentigines, atrial myxoma, mucocutaneous myxoma, and blue nevi) and NAME (nevi, atrial myxoma, myxoid neurofibroma, and ephelides) syndromes.8 Myxomas in patients with Carney complex account for 7% of all cardiac myxomas, are typically found at a younger age, and may have higher recurrence rates.4,13 Hamartomas, rhabdomyomas, and fibromas are diagnosed almost exclusively in children.14 Rhabdomyomas are the most common pediatric cardiac tumor and are associated with tuberous sclerosis.
Malignant primary tumors comprise the remaining 25% of cardiac neoplasms. Primary malignancies of the myocardium comprise the bulk of the remaining cases, of which sarcomas account for the vast majority. Malignant fibrous histiocytoma, angiosarcoma, fibrosarcoma, and rhabdomyosarcoma are among the more common histologic types.15 Table 54.1 summarizes the relative frequency of specific subtypes of sarcoma that may be diagnosed. The median age at diagnosis is 30 to 40 years, slightly younger than that for benign tumors, and there is no sex predilection as seen in myxoma.15 Lymphomas account for only about 2% of primary cardiac tumors, but the incidence appears to be increasing.16 Melanoma and carcinoma may also occur infrequently.
Primary malignant tumors of the pericardium are exceedingly rare and include mesothelioma, fibrosarcoma, angiosarcoma, and malignant teratoma.17 An American Medical Association survey of nearly 500,000 autopsies revealed a 0.0022% incidence of primary malignant pericardial neoplasms.18 It appears that malignant mesothelioma is the most common primary malignancy of the pericardium, accounting for 50% of primary pericardial tumors. Asbestos has well-established associations with pleural and peritoneal mesothelioma, and there appears to be some correlation in pericardial mesothelioma.19 Unfortunately, due to the low incidence, this association has been inconsistent, and no other risk factors have been identified.20–22 There have been very few cases reported since 1994, when 140 cases had been reported in the literature.17,18,20–26 Fibrosarcoma, angiosarcoma, synovial sarcoma, and teratoma of the pericardium have also been documented.17,21,26
With advances in echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI), the postmortem diagnosis of cardiac tumors is becoming less common. Surgical series seem to demonstrate an increase in the ratio of benign to malignant tumors, with malignant tumors accounting for only 10% of cases in a narrow range of 6% to 20%.14,27–32 This is likely the result of surgical management of benign myxoma, which accounts for over 80% of patients in some series, combined with changes in patient selection.27,28,31
The majority of primary cardiac tumors arise in adults with a median age of 45 to 55 years, but can be seen at any age.14,27–32 Among 533 cases in the database of the Armed Forces Institute of Pathology, McAllister and Fenoglio7 noted that 83% of patients were adults. Infants (<1 year of age) comprised 9% of the patients and, in this group, 96% of tumors were benign and only 4% were malignant. In a review of the data from the National Cancer Institute Surveillance, Epidemiology, and End Results from 1973 to 1987, Mack15 reported no sex predilection for the incidence of sarcoma of the mediastinum and heart.
Metastatic disease to the heart and pericardium occurs at a frequency much greater than that of primary tumors.33–39 In a review of more than 12,000 autopsies in Hong Kong, Lam et al.37 noted that cardiac metastases were over 20 times more common than primary tumors and may be present in up to 20% of patients dying of disease. The majority of cases have involvement of the pericardium, whereas myocardial involvement is uncommon. In a review of autopsy series of patients with a known malignancy, Hanfling35 noted the rate of reported cardiac involvement increased steadily from 1.5% in the late 1800 s to 18.3% in 1960. Contemporary series indicate the rate of cardiac metastases in patients dying of cancer may be as high as 20%.7,35–38,40,41
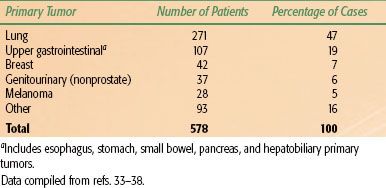
The sites of origin of cardiac metastases from solid tumors are summarized in Table 54.2. Lung cancer is the most common cause of cardiac metastases and accounts for nearly one-half of all cases. Upper gastrointestinal malignancies and breast cancer are also common causes of cardiac metastases, accounting for one-fourth of all cases. The remaining one-fourth of cases arise from a wide variety of other malignancies.33–38 Melanoma is purported to have the highest propensity for metastatic spread to the heart and tends to involve the endocardium or myocardium, with some series showing its incidence of cardiac metastases rivaling or exceeding that of lung cancers.2,41 Cardiac metastases may also originate from lymphoma or leukemia. In 1960, Hanfling35 reported that the proportion of cardiac metastases arising from these malignancies rivals that arising from solid tumors. However, multiple medical advances in both chemotherapy and diagnosis have occurred since then, and modern series consistently report that these histologies account for approximately 17% of cardiac metastases.33,34,36,37
Tumors of the GV are extremely rare. The literature on these consists mainly of case reports, and approximately 130 cases have been documented. As a whole, tumors of the GV are about as common as primary malignant pericardial mesothelioma. The largest series has been reported by Burke and Virmani.42 They evaluated 45 tumors on the files of the Armed Forces Institute of Pathology and found that all of the tumors were sarcomas, including intimal (undifferentiated) sarcoma, angiosarcoma, leiomyosarcoma, and synovial sarcoma. There appeared to be no sex predilection for tumors of the aorta or pulmonary artery, although the female-to-male ratio was 3 to 1 among patients with tumors of the IVC.
TABLE 54.2 SITE OF ORIGIN FOR CARDIAC METASTASES
 NATURAL HISTORY
NATURAL HISTORY
Tumors of the Myocardium
Myxomas, as discussed previously, are the most common benign tumors of the heart, are seen in women twice as frequently as men, and are diagnosed at a mean age of 45 to 55 years, but have been documented in infants and octogenarians.27–32,43 Benign myxomas tend to be slow growing and are minimally invasive and as such may have a long duration of symptoms before diagnosis. Typically, these tumors arise from the interatrial septum and grow into the adjacent chamber. The left atrium is the most common site of involvement for myxoma, and this is 6 to 7 times more common than myxoma of the right atrium. The tumor may also be located in the ventricles or the valves and can be bilateral. Although they are considered benign, the tumor can elicit dramatic symptoms from valvular insufficiency, congestive heart failure, and embolic phenomena. Surgical excision is the treatment of choice, with local recurrence rates ranging from 0% to 5.4%.8
Primary malignant tumors of the myocardium, most commonly sarcomas, do not show a predilection for site of the tumor in the heart, except for angiosarcomas, which tend to occur more frequently in the right atrium, and often present late with advanced disease and lung metastases.14,27,28,30,31 The duration of symptoms is on the order of months, and survival is poor. Even after attempts at curative resection, recurrences are common, and the median survival ranges from 6 to 18 months.14,27–32,44,45 The cause of death is most often complications of locally recurrent disease with invasion of adjacent chambers, valves, or pericardium. Tamponade, hemopericardium, and distant metastases are common.45 About 30% of primary cardiac sarcomas have distant metastases at the time of diagnosis.2 The high incidence of hematogenous dissemination of a cardiac sarcoma may be explained by the high rate of blood flow through the heart.46
Tumors of the Pericardium
Mesothelioma is the most common pericardial neoplasm and may either be confined to the pericardial sac at diagnosis or extend beyond it, involving the myocardium or mediastinal structures.20–22 Of 140 primary malignant pericardial mesotheliomas reported in the literature, only 28% of cases were diagnosed antemortem.21 These tumors have been documented to metastasize by lymphatic and hematogenous routes to involve regional lymph nodes, lung, liver, brain, bone, and adrenal glands.17,18,20–25 Despite the metastatic potential, pericardial tumors are more often fatal because of local complications, such as restrictive pericarditis with resultant cardiac tamponade, arrhythmia due to myocardial invasion, or vena caval obstruction. Even if the tumor can be diagnosed antemortem, survival is poor. Typically, the onset of symptoms does not occur until the tumor is well advanced, and from that time the median survival is <6 months, with only a handful of patients surviving beyond 1 year.23–25
Tumors of the Great Vessels
The median age at presentation is 40 to 60 years for tumors of the GV.42 The natural history and clinical presentation depend on the exact location of the primary tumor. Depending on the location, symptoms may include dyspnea, cough, hemoptysis, pain, and thromboembolic phenomena, including pulseless extremities, stroke, peripheral edema, and superior vena cava (SVC) syndrome. In the series by Burke and Virmani,42 they found that in contrast to the tumors of the aorta and pulmonary artery that were aggressive sarcomas arising from the vessel lumen, tumors of the inferior vena cava (IVC) were mostly low-grade leiomyosarcomas originating from the medial layer of smooth muscle in the vessel wall.
TABLE 54.3 SCOPE OF CLINICAL MANIFESTATIONS OF CARDIAC TUMORS
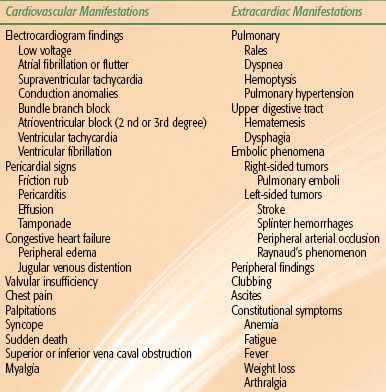
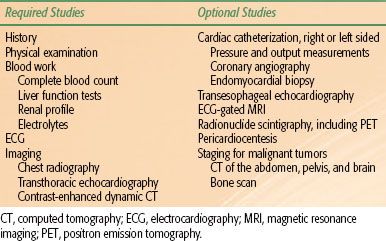
TABLE 54.4 DIAGNOSTIC EVALUATION FOR A SUSPECTED OR KNOWN CARDIAC TUMOR
 DIAGNOSIS
DIAGNOSIS
Tumors of the heart have been referred to as the “great imitators” of the cardiovascular system, and although there are no pathognomonic signs or symptoms, cardiac tumors can often be detected through careful attention to both cardiac and extracardiac manifestations of the disease.47,48 It is not surprising that tumors of the heart are often asymptomatic until they become advanced enough to affect blood flow or cardiac function.35 As the tumor enlarges, disturbances in normal heart function produce different signs and symptoms depending on the location of the tumor. The scope of clinical presentation is summarized in Table 54.3. Tumors involving the right heart may result in pulmonary emboli, pulmonary hypertension, tricuspid valve disease, or SVC or IVC obstruction. Left-sided tumors can cause mitral valve disease, thromboembolic phenomena, and rapidly progressive congestive heart failure, which may be refractory to treatment. A characteristic auscultation finding referred to as a tumor plop may be heard during early diastole in 30% of patients.49 Arrhythmias are very common and are predominantly supraventricular tachycardia or nonspecific conduction anomalies.48 Specific presenting complaints are equally varied. Dyspnea is the most common presenting complaint and is noted in 59% to 88% of patients.33,44,50,51 Palpitations or syncope is also seen frequently, may be positional, and, if the tumor obstructs a valve orifice, sudden death may result. Chest pain can be anginal, resulting from direct myocardial invasion or obstruction of the main coronary ostia. It can also be sharp, due to invasion of the pericardium, with resulting pericarditis. Constitutional symptoms also occur, with fever, malaise, anemia, and weight loss.33,35,44,48,50,51 Tumors of the pericardium and GV show a similarly variable constellation of symptoms, and as such, they pose the same diagnostic difficulties as tumors of the myocardium.
Physical examination may reveal tachycardia, murmur (which may be positional), pericardial rub, gallops, peripheral edema, jugular venous distention, rales, and stigmata of thromboembolic disease. Electrocardiography (ECG) most often reveals nonspecific ST- and T-wave changes, although low-voltage ECG, supraventricular tachycardia, bundle-branch block, or second-degree (type II) or third-degree atrioventricular node block may also be noted. Laboratory studies may reveal anemia, erythrocytosis, thrombocytosis, thrombocytopenia, leukocytosis, and elevated erythroid sedimentation rate.44,48,51,52
 DIAGNOSTIC WORKUP
DIAGNOSTIC WORKUP
Before the advent of echocardiography and angiography, 66% of tumors were diagnosed intraoperatively during exploration for suspected valvular disease. With current techniques, the diagnosis can be made reliably in the preoperative setting in almost 90% of cases.27 The diagnostic evaluation of patients with suspected cardiac tumors is presented in Table 54.4.
Physical examination and ECG findings have been described above. The imaging techniques used in the diagnosis and evaluation of cardiac tumors include chest radiography, CT, MRI, echocardiography, radionuclide scintigraphy, and cardiac catheterization. Although there is considerable overlap among these studies, each modality is unique and complements the others in evaluating the tumor. Chest radiography shows abnormalities in over 80% of patients. Unfortunately, abnormalities are usually nonspecific and therefore of limited usefulness. Findings include cardiomegaly, an abnormal cardiac contour, mediastinal widening, or evidence of congestive heart failure.48,53,54 Calcifications are present in up to 20% of cases, perhaps relating to the presence of valvular or pericardial disease.53,55 Calcifications on imaging may also suggest the presence of a fibroma. In the setting of a malignant tumor, chest radiography may also reveal hilar nodal, pulmonary, or osseous metastatic disease.
Echocardiography, M-mode and two-dimensional, is the diagnostic procedure of choice among patients with suspected cardiac tumors. Either transthoracic (TTE) or transesophageal (TEE) techniques can be performed, yielding valuable information regarding size, shape, location, mobility, and areas of attachment.48 In a review of 533 primary cardiac tumors, Blondeau27 found echocardiography provided a 98% diagnostic accuracy rate among the 437 patients for whom it was used. Bogren et al.54 found that echocardiography detected abnormalities in 63 of 65 (97%) patients with primary cardiac tumors. With this high level of diagnostic yield, and because the use of TTE has no known side effects, it should be performed for all patients. TEE is a complementary procedure to TTE. It is a more invasive procedure and is not required in all patients, but it may be used for guidance during endomyocardial biopsy and may also provide better evaluation of the left atrial appendage and right-sided tumors.56–58
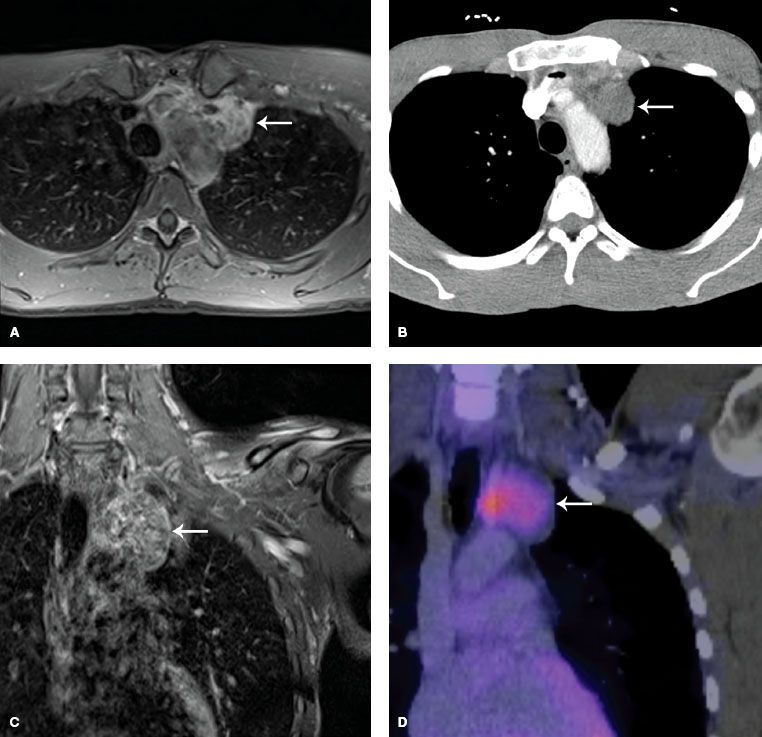
FIGURE 54.1. Axial contrast-enhanced fat-saturated T1 magnetic resonance image (MRI) of a primary cardiac neoplasm arising from the left atrium (A); corresponding axial contrast-enhanced computed tomography (CT) (B), coronal contrast-enhanced fat-saturated T1 MRI (C), and coronal fluorodeoxyglucose positron emission tomography CT (D) images. Tumor indicated by white arrows.