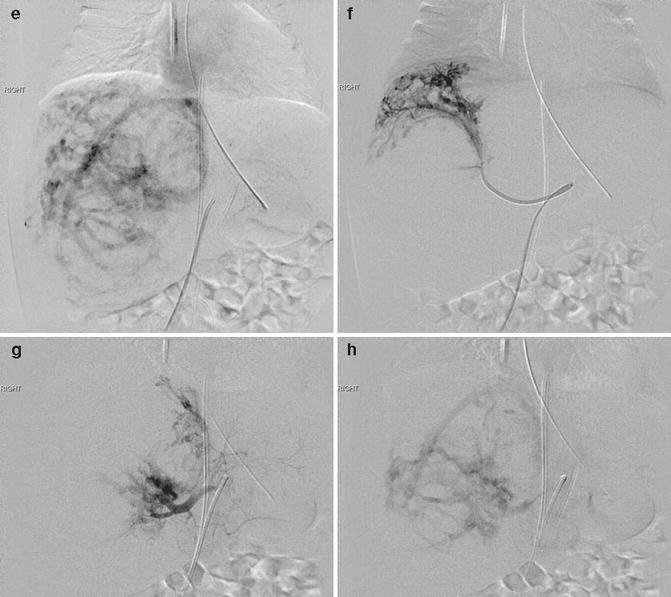
Fig. 15.1
Term neonate requiring mechanical ventilation and pressors with cardiac volume overload and respiratory insufficiency due to massive hepatic RICH. Hepatic arterial supply was partially embolized using large particles and Gelfoam, resulting in rapid clinical improvement. The infant was extubated and feeding normally within 2 days of the procedure and continues to do well. (a) T2-weighted coronal MRI shows a large spherical heterogeneous mass in the right hepatic lobe. (b) Color Doppler ultrasound image of the liver shows dilated hepatic vessels with a low-resistance Doppler waveform consistent with arteriovenous shunting. (c) MR angiography shows the extreme vascularity of the mass. (d, e) Hepatic arteriogram confirms the high-flow nature of the focal lesion, without direct arteriovenous fistulae. (f) Segmental angiogram prior to embolization. (g, h) Hepatic angiogram carried out after embolization shows subtotal occlusion of the tumor vascularity. If the patient did not improve, further embolization could be carried out in a second stage. RPHA, right posterior hepatic artery
Summary
Embolization is generally not a first-line treatment for infantile and congenital hemangiomas, as well as kaposiform hemangioendotheliomas, but can be effective and even lifesaving in selected situations.
References
1.
2.
3.
Burke DR, Verstandig A, Edwards O, Meranze SG, McLean GK, Stein EJ (1986) Infantile hemangioendothelioma: angiographic features and factors determining efficacy of hepatic artery embolization. Cardiovasc Intervent Radiol 9(3):154–157CrossRefPubMed
Related posts:
 Hemangiomas of Infancy: Epidemiology
Epidemiology of Vascular Malformations
Hemangiomas of Infancy: Epidemiology
Epidemiology of Vascular Malformations
 Surgery of Hemangiomas
Surgery of Hemangiomas
 Dermatological Manifestations of Vascular Malformations
Dermatological Manifestations of Vascular Malformations
 Classification of Arteriovenous Malformation and Therapeutic Implication
Classification of Arteriovenous Malformation and Therapeutic Implication
 Vascular Malformations of the Limbs: Treatment of Venous and Arteriovenous Malformations
Vascular Malformations of the Limbs: Treatment of Venous and Arteriovenous Malformations
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


