THYROID NEEDLE ASPIRATION AND BIOPSY
Part of “CHAPTER 39 – THE THYROID NODULE“
Obtaining tissue or cells from a thyroid nodule by some form of biopsy technique is the best single method to identify malignancy.68,69 and 70 Biopsies can be performed by fine-needle (22- to 27-gauge) aspiration (FNA), large-needle (16- to 18-gauge) aspiration, or cutting-needle biopsy (14-gauge Tru-Cut or Silverman needle). Most clinicians have found FNA to provide the highest incidence of successful samples and the lowest incidence of complications while yielding a diagnostic precision equal to or better than that of other methods.2 This technique is shown in Figure 39-1. In selected large lesions for which FNA has failed to provide a satisfactory diagnosis, some other aspiration method may be used.
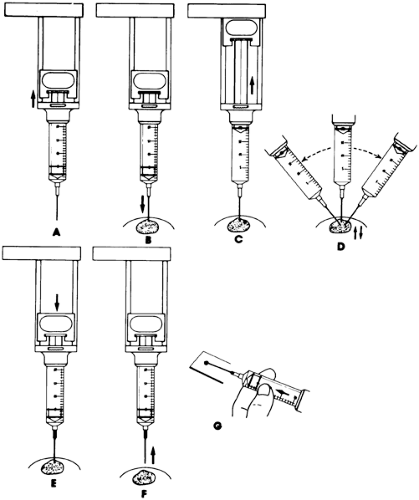 FIGURE 39-1. Technique for fine-needle aspiration biopsy. A, Aspirate 1 to 2 mL of air into syringe to loosen plunger and facilitate expiration of contents after aspiration. B, Insert needle into lesion without aspiration. C, Retract syringe piston to provide maximum suction. D, Make several passes at different angles, withdrawing needle to near the surface before redirecting. E, Release suction passively. F, Withdraw needle. G, Express needle contents onto a glass slide. |
FNA has been popular in Europe for decades and now has attained similar acceptance in the United States. The ability to obtain adequate samples improves with experience, and the success rate approaches 95%. However, the collecting technique appears less critical than the ability of the pathologist to interpret the cytologic specimens correctly. Because of these two primary factors, this procedure is best limited to situations in which the operator and pathologist each have considerable experience.71,72 and 73 Ultrasonography-guided FNA has proven a useful technique for biopsy of low-lying nodules or those that are detected by ultra-sonography but are difficult to palpate.74,75
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


