Thyroid
ANATOMY
The thyroid gland consists of the right and left lobes joined by an isthmus, which crosses the trachea at the second or third cartilaginous ring; a pyramidal lobe may extend superiorly from the isthmus or one of the thyroid lobes (Figs. 21-1 and 21-2).
NATURAL HISTORY
Thyroid cancer represents approximately 2% of all malignancies and accounts for less than 1% of cancer deaths in the United States (14).
There were estimated to be 37,200 new cases in 2009 (10,000 males and 27,200 females) and 1,630 deaths (690 males, 940 females) (1).
Thyroid exposure to radiation, particularly before puberty, is the only well-documented etio-logic factor: 25% of persons who receive 0.02 to several Gy of external irradiation develop goiters, and 25% of these, or 7% of all persons who receive thyroid irradiation, develop cancer, usually papillary adenocarcinoma (6). In two studies of patients with tonsillitis treated with x-rays, thyroid cancer developed in 6% and 7%, respectively (5).
A linear, no-threshold model suggests that with less than 2,000 rem of external irradiation, children have absolute risks for thyroid cancer or nodules of 4.2 and 12.3 cases per 106 persons per rem per year, respectively (9).
DIAGNOSTIC WORKUP
No single factor, physical finding, or laboratory test is pathognomonic for detection of thyroid cancer, with the exception of serum calcitonin level for medullary thyroid cancer.
Standard radiographs: The most common feature associated with thyroid nodules is intraglandular calcification.
Radionuclide imaging:131I,125I,123I, and99mTc are most commonly used for thyroid imaging. Indications for imaging in suspected or proven thyroid cancer include anatomic and functional evaluation of palpable thyroid nodule, detection of occult or minimal cancer in highrisk patients, detection of primary tumor in a patient with known regional or distant thyroid metastases, detection of metastases, and assessment of therapeutic effects. Approximately 15% to 25% of single cold nodules are cancers; the other 75% to 85% are adenomas or colloid cysts.
Ultrasonography: Ideally, ultrasonography is performed with a high-resolution, high-frequency (7.5 to 10.0 MHz) transducer (14). A cold nodule less than 4 cm in diameter on radionuclide imaging that appears cystic on ultrasound has less than 0.5% probability of being malignant, whereas a solid nodule on ultrasound has a 30% probability of being malignant.
Fine-needle aspiration biopsy: Best results are obtained with 1- to 3-cm nodules. This technique differentiates benign from malignant nodules and has as high as 95% accuracy (7).
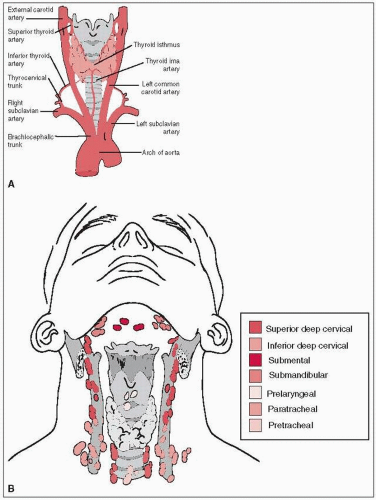 FIGURE 21-1 Anatomy (A) and lymphatic drainage (B) of the thyroid. (A: From Agur AMR, Dalley AF, eds. Grant’s atlas of anatomy, 12th ed., Philadelphia, PA: Lippincott Williams & Wilkins, 2009:770; B: From Wolters-Kluwer collection 4206.008.024.eps, with permission.) |
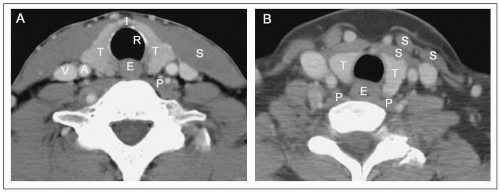 FIGURE 21-2 Important anatomical relations of the normal thyroid gland in two separate patients on CT imaging. A: Section at the level of the isthmus (I). B: Section just above the isthmus. Note that the thyroid gland (T) overlies the tracheal ring (R) and the lobes are in direct contact with the strap muscles (S) anteriorly and anteriolaterally. The lobes also abut the prevertebral muscles (P) posteriorly, the esophagus (E) posteriomedially, and the common carotid artery (A) and the internal jugular vein (V) laterally. (Chao KSC, Apisarnthanarax S, Ozyigt, G. Practical essentials of intensity modulated radiation therapy. Philadelphia, PA: Lippincott Williams & Wilkins, 2003:211.) |
STAGING SYSTEM
The American Joint Committee on Cancer staging system (2) for carcinoma of the thyroid is shown in Table 21-1.
PATHOLOGIC CLASSIFICATION
Differentiated Thyroid Cancer
Differentiated thyroid cancer consists of papillary, mixed papillary-follicular, and follicular adenocarcinoma.
It arises from thyroid follicular cells (endodermal origin) and can be treated with131I and thyroid hormone suppression.
Papillary cancer (including mixed papillary-follicular) represents 33% to 73% of malignant thyroid lesions and more than 90% of thyroid neoplasms found incidentally at autopsy. It occurs mostly in the third to the fifth decades and is 2 to 4 times more common in women than in men.
Follicular cancer represents 14% to 33% of primary thyroid tumors and affects women 2 to 3 times more frequently than men. Average age at diagnosis is 50 to 58 years; it is rarely seen in children.
Medullary Thyroid Cancer
Medullary thyroid cancer is derived from parafollicular or C cells that arise from the neuroec toderm; it accounts for 5% to 10% of all thyroid cancers.
Anaplastic Cancer
Anaplastic cancer represents approximately 10% of all malignant thyroid lesions.
Patient age ranges from 40 to 90 years, and women outnumber men four to one.
Eighty percent of patients have a history of goiter.
TABLE 21-1 American Joint Committee Staging System for Carcinoma of the Thyroid | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||