Summary of Key Points
† Deceased.
- •
To describe the functions of advocacy.
- •
To describe how lung cancer advocacy groups accomplish their goals.
- •
To describe how they can influence lung cancer outcomes.
Advocacy is defined as the act or process of supporting a cause or proposal. Effective advocates in the health-care field influence disease awareness and education, research and drug development, public policy, and legislative and governmental issues. Cancer advocates have become an instrumental and influential force on behalf of cancer care.
Cancer advocacy is rooted in the early work of the breast cancer movement in the United States beginning in the 1970s. The political and social activism of the HIV/AIDS movement during the 1980s and 1990s further influenced US breast cancer advocacy. Foundations and charitable organizations emerged to fund efforts on behalf of breast cancer information, education, emotional support, and research. Media played an essential role, and with an engaged public, policymakers and decision makers were paying attention to the vision and demands of the breast cancer advocacy community, which eventually led the way for advocacy efforts for other disease types. The common goals of cancer advocates include raising awareness and education; ensuring patient access to screening, diagnosis, and treatment; stimulating research and clinical trials; addressing the psychosocial and emotional issues associated with cancer; and empowering individuals to gain control of their disease. Advocates are directly responsible for challenging public perceptions, stigma, and disease identity; they can influence and shape research and policy agendas.
Today, in many parts of the world, cancer advocates work in conjunction with medical experts, political leaders, the pharmaceutical and biotech industries, corporations, and government and legislative representatives. Each country and region of the world presents unique issues for advocates that are based on culture, society, economics, and existing governmental and health policy infrastructures. Global patient advocacy must tailor its tactics and activities to meet and respond to these needs.
Lung Cancer Advocacy Groups
In 2001, a global search revealed the existence of only nine not-for-profit organizations with an interest in lung cancer advocacy. Of these, only two were lung cancer specific; the others were representing generic cancer or respiratory diseases. In coming together, these organizations established the Global Lung Cancer Coalition (GLCC), an allied group of registered not-for-profit, nongovernment organizations dedicated to improving lung cancer outcomes. By 2016, the GLCC had grown to 35 member organizations, from 25 countries, and now provides a centralized referral network to these organizations within its website. Lung Cancer Europe is a relatively new coalition, which provides a European platform for already existing lung cancer patient advocacy groups and supports the establishment of new national groups in European countries, where they do not currently exist. More information is available at http://www.lungcancereurope.eu . There are also additional lung cancer advocacy groups in the United States, and there may well be others across the world advocating in this disease.
Challenges in Lung Cancer Advocacy
Despite the recent formation of several advocacy groups in lung cancer, the number of these groups is still low. Lung cancer advocacy is most developed in North America, Australia, and the European Union, in particular, the United Kingdom. We see small groups emerging elsewhere in the world, even though in Eastern Europe national lung cancer organizations are not common. As with other health-related agendas, sustaining and building advocacy groups is a challenge. Negative issues associated with lung cancer, such as those described in the following section, make it particularly difficult to advocate for change and improvement.
Lack of Advocates
Individuals who advocate for a particular disease tend to be directly affected by the disease, such as patients and caregivers. Sadly, few people with lung cancer are well enough or survive long enough to become advocates. Lung cancer is the number 1 cancer claiming more lives than any other cancer in the world and has a less than 17% 5-year survival rate. An additional issue is that compared with other common cancers, there are relatively few high-profile celebrity supporters of this disease. As such, there are relatively few lung cancer voices championing the cause.
Stigma Surrounding the Association With Tobacco
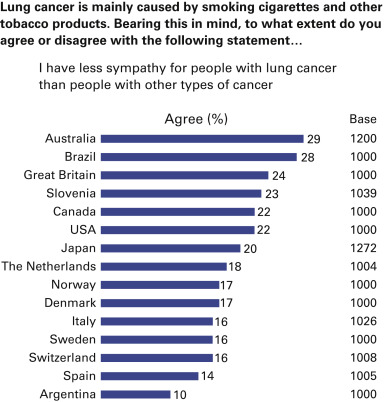
Lung cancer is often seen as self-inflicted because of its association with tobacco. An Ipsos MORI consumer poll, commissioned by the GLCC in 2011, showed that, although there was national variation across the 15 countries surveyed, on average, 20% of people felt less sympathy for people with lung cancer than for people with other common cancers ( Fig. 61.1 ). The national variation was 10% to 29%.
People with lung cancer have reported higher levels of perceived cancer-related stigma compared with people with breast or prostate cancer. The belief that one has caused one’s own cancer has been correlated with higher levels of guilt, shame, anxiety, and depression. The stigma caused by a tobacco-related disease can create hardship for patients, many of whom suffer in silence and isolation and feel a sense of hopelessness and helplessness about their condition. In fact, irrespective of whether people with lung cancer smoked or have never smoked, they feel stigmatized because of the tobacco association.
The stigma and blame associated with lung cancer are also a contributing factor to late presentation. Stigmatization has a negative impact on the disease and on advocacy initiatives. Central to the lung cancer advocacy community is its focus on reducing the stigma associated with this disease because it can profoundly affect not only patients in their personal identity, social life, and economic opportunities, but also their families. Many diseases are lifestyle related, yet the patients are not affected in this way. It is important that messages such as “no one deserves lung cancer” and “smoker, former smoker, or never-smoker—anyone can get lung cancer” are widely disseminated.
Low Public Profile
Because of poor outcomes overall, a lack of advocates, and a relative lack of celebrity supporters, engaging the media in lung cancer has been challenging. Journalists in many countries consider lung cancer to be depressing and so have been reluctant to report on lung cancer issues. In addition, there is a reluctance from those living with lung cancer to speak out, given the stigma and fear of self and community blame.
Lung Cancer Advocacy Group Activity
All organizations engaging in lung cancer advocacy are different and respond to the particular culture and need of their regions or countries. However, they campaign for some or all of the following.
Integrated Tobacco Control Programs
Many lung cancer advocacy groups have an interest in disease prevention and campaign for the development and implementation of antitobacco strategies. These strategies include smoking cessation services; legislation, where necessary (e.g., to ban smoking in enclosed public places, point-of-sales advertising, cigarette vending machines, and to ensure plain packaging for cigarette packs); educational programs in schools; and public awareness campaigns, all of which underscore the importance of not smoking and the value of quitting.
Increased Funding for Lung Cancer Research
Globally, lung cancer is the most common cancer. Yet, compared with other common cancers, there has been relatively little investment in lung cancer research. The GLCC has commissioned the Institute of Cancer Policy to undertake a review of “The State of Global Lung Cancer Research.” As many as 32,000 published lung cancer research articles were examined, from 2085 different journals. Of these, only 5.6% of all global cancer research was in lung cancer (2013), an increase of only 1.2% since 2004. As many as 24 countries were found to be responsible for more than 95% of lung cancer research outputs. Individual country reports are available at http://www.lungcancercoalition.org . The majority of lung cancer research (53%) is focused on medicines, genetics, and biomarkers, with only 1% on supportive and palliative care issues.
In 2013, the National Cancer Research Institute reported that only 6.7% of cancer site-specific spending in the United Kingdom was on lung cancer (charities and government). Although this rate represents an increase from the 3.9% spent on lung cancer in 2006, the rate is still poor despite the fact that lung cancer accounts for more than 20% of cancer deaths in the United Kingdom annually.
In 2015, Cancer Australia reported that only 5% of cancer site-specific spending in Australia was on lung cancer (charities and government). Total funding to lung cancer research (including pleural mesothelioma) decreased from 2006−2008 to 2009−2011 and showed that the proportional funding to lung cancer research was very low compared with incidence, mortality, and burden of disease on the Australian population. Lung cancer accounts for 19% of cancer deaths in Australia annually.
Campaigning to increase investments in lung cancer research is a core function of lung cancer advocacy. Many lung cancer advocacy groups are also funders of research, working in conjunction with scientists and clinicians to build research capacity in the lung cancer community to ensure better future outcomes.
Increased Number of People With Lung Cancer Enrolled in Clinical Trials
Unless a person with lung cancer is being treated at a center that participates in clinical trials relevant to his or her disease, it can be very difficult to access clinical trials or even be aware of them. Many advocacy groups play a key role in this area, both in raising awareness of clinical trials in general and in directing people with lung cancer to appropriate trials and trial sites. Some advocacy groups have included links to clinical trial databases from their websites to make it easier for people with lung cancer to find appropriate trials; the lack of a national service that can provide adequate and updated information is a barrier for people who wish to participate in clinical trials. The GLCC has also collated links to websites in various countries, where details on clinical trials are available.
Earlier Diagnosis
Diagnosing more people with lung cancer at an early stage, when curative treatments are an option, can save lives. In recent years, there has been increased focus on lung cancer screening. In countries where lung cancer screening is available, advocates are directing high-risk individuals to these services. Advocates are also calling for further research to evaluate the benefit of screening tools.
Raising general public awareness of the signs and symptoms associated with lung cancer is a key function of many lung cancer advocacy groups; however, there is a variety of associated signs and symptoms, so this can be a difficult task. In England, the Department of Health, in 2012, funded the national “Be Clear on Cancer—Lung Cancer” campaign. This campaign, focusing on persistent cough, and results from the pilot study noted a 22% increase in the number of patients who visited their general practitioner with relevant symptoms and also noted an increase in chest computed tomography scans being performed. This campaign was repeated in 2013 and in 2014. Results of the 2012 campaign showed that an extra 700 diagnoses were made (9% higher than same period in 2011) and around 400 patients were picked up in early stage (300 of whom were offered surgery). Using nationally agreed-upon guidelines, advocacy groups have produced community information such as the GLCC awareness-raising leaflets, which are translated into 13 languages and available for download.
Equitable Access to Best-Practices Treatment and Care
Ensuring equitable access to the best care is of ever-increasing importance in lung cancer advocacy because of current global financial issues, pressures on health services budgets, and the rising cost of new diagnostics and therapies. It is the advocate’s ultimate goal that all people with lung cancer will be treated within nationally agreed-upon treatment guidelines, that they will be offered high-quality support and information, and that they will have access to up-to-date, evidence-based diagnostics and therapies. Across regions and countries of the world, realistic expectations vary. However, using the Internet and social media, people with lung cancer are able to learn about available lung cancer treatments and technologies, but may not be able to access them, which may result in considerable distress.
The production of patient-focused information materials on all aspects of lung cancer diagnosis, treatment, and care is a core function of most advocacy groups. Such information ensures that patients and their families have a better understanding of their disease and are better equipped to make informed decisions about care. Some advocacy groups have positioned themselves as an extension to the health-care system and a supportive care service for patients and caregivers whilst away from their treating centers. Information can be delivered in many formats, such as print, the Web, DVD, and other new media formats. A challenge for all patient information providers is to ensure that these materials are current, evidence based, and easily accessible.
In recent years, financial pressures across the globe have resulted in health-care providers undertaking formal health technology assessments, particularly in the area of new developments, including targeted therapies and immunotherapies. Cancer advocacy groups play a substantial role in making sure that national health technology assessment bodies understand the importance of segmented populations, biomarkers, and issues of study crossover. In this new research area, in particular in the United States, cancer advocacy groups have taken on a key role in tissue banking and molecular testing; the National Lung Cancer Partnership has collaborated with 14 top cancer centers to form the Lung Cancer Mutation Consortium, which is the largest effort to date to promote molecular testing for people with lung cancer. Elsewhere, groups are raising awareness of new lung cancer diagnostics, evidence-based clinical pathways, and campaigning for widely available pathology services.
High-Quality Data
Underpinning all issues is the need for advocates to access high-quality, timely data on survival, quality of life, and patient experience. Such data not only provide a benchmark for the quality and outcomes of lung cancer services, but also give advocates a tool with which they can campaign for improvement and showcase best practices. A good example of this is the work of the International Cancer Benchmarking Partnership, which has shown a huge variation in 1-year and 5-year survival rates in lung cancer across the study countries, prompting health-care policymakers to investigate reasons for these differences.
In November 2015, the GLCC launched a global interactive lung cancer altas, allowing clinicians and advocates to easily source and compare lung cancer data from every World Health Organization (WHO) country. Data available include mortality, incidence, survival, and other country-specific data on cancer registry, cancer planning, and implementation of the WHO Framework Convention on Tobacco Control.
An important national initiative is the United Kingdom’s National Lung Cancer Audit. Year after year, this audit has shown improvement in areas such as the rate of surgical resection. These audit data have been extensively used by advocacy groups in the United Kingdom, as in the Web-based Smart Map, which displays the data in a patient-friendly, easily accessible format. Elsewhere, a European Respiratory Society taskforce has completed a feasibility study regarding the prospective collection of clinical data for people with lung cancer in 27 European countries. Their hope is that a Pan-European database of people with lung cancer can soon be a reality.
Help for People With Lung Cancer and Their Families
Living with the disease, the diagnosis, and treatment of cancer are traumatic events for people with cancer and their loved ones. It can be a time of a great emotional distress and can evoke a wide range of emotions. The expression of these feelings is crucial in order to cope with a diagnosis of cancer and side effects from treatment; emotional support, physical care, and practical help may be of benefit to both patients and their families.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


