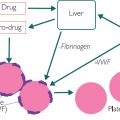
Figure 8.1: A normal response to a viral infection
In Figure 8.1, the virus uses the internal machinery of the cell to replicate itself. It then bursts the cell and infects an adjacent cell. Because the virus is small (compared to bacteria), the cell needs to make the white cells aware that it has been infected.
Storytelling: The virus inside the infected cell is too small to be detected by the white cells. The infected cell spreads the news of the infection to the white cells by taking a small part of the virus, called an antigen (Ag), and ‘placing it on a stick’ outside the cell. This stick is called major histocompatibility complex (MHC). The T cell (a type of lymphocyte) then acts like a camera and takes a picture of the MHC/Ag. Having taken the photo, the T cell uses it to make a ‘Wanted poster’ of the MHC/Ag ‘villain’ and shows the poster to the B cell (a type of lymphocyte). The B cell makes antibodies (Ab) specifically designed to counteract the Ag, and the tailor-made Ab binds itself to the Ag. Once bound, a signal is activated and this attracts a ‘posse’ of neutrophils, natural killer cells and CD4/CD8 cytotoxic T cells to destroy the cell hosting the villainous virus.
The process of destroying the virus usually causes cellular damage. It increases C-reactive protein (CRP), produces more neutrophils and plasma viscosity (PV), and raises WBC (white cell or lymphocyte count). For example, human immunodeficiency virus (HIV) destroys the T cells and so the lymphocyte count may actually go down. With the T cell ‘camera’ not working, AIDS patients may be susceptible to otherwise benign viral infections.
This can also be seen when diagnosing viral hepatitis. For example, the presence of hepatitis B surface antigen (HepBsAg) may indicate a current infection. Likewise, the presence of HepB Ab will suggest a live infection (if HepBsAg is also present), a successful vaccination, or the presence of the disease in the past (as the B cells have made a specific Ab for HepB). There is also a new, rapid technique available that measures the DNA or RNA of the HepB virus directly in the cell. This is helpful in children or acute cases, as it may otherwise take a few days or even months for the patient to produce enough Ag or Ab to be measured ( the hepatitis virus that damages the hepatocyte, which often increases the liver enzyme ALT).
the hepatitis virus that damages the hepatocyte, which often increases the liver enzyme ALT).
Autoimmune basics
In autoimmune conditions, there is no viral infection. But for some reason (which is still unclear at present), a part of the cell’s own protein is placed ‘on the stick’. This causes the same chain of events, which leads to the production of a specific antibody. Broadly, for rheumatoid arthritis this Ab is rheumatoid factor (RF); for ankylosing spondylitis (AS) it is HLAb27; for pernicious anaemia it is parietal cell Ab or intrinsic factor Ab; and for systemic lupus erythematosus (SLE) it is anti-nucleic antibody (ANA).
There are hundreds of possible Ab tests, usually undertaken in secondary care by a consultant. If the Ab is present then the patient is called ‘seropositive’; if it is not present then the patient is labelled ‘seronegative’. For most Ab tests, about 80% of people with the symptoms are seropositive, leaving 20% seronegative. For these seronegative patients, we could undertake more Ab tests. However, in practice it’s more likely that their symptoms will be treated as if they were positive and the effects reviewed. The reason for the existence of symptoms in seronegative patients is unclear.
As discussed in the case study in Chapter 4, autoimmune patients may have blood tests to consider the autoimmune diagnosis (RF), white cell and inflammation response to the condition (WBC, neutrophils, CRP, PV) and any effects of treatments or interventions (RBC, MCV, folate, LFTs and U&Es).
There are also antibodies, called anti-neutrophil cytoplasmic antibodies (ANCA), which ‘attack’ and then change the role of neutrophils. They are commonly associated with vasculitis, which is the inflammatic destruction of the vasculature; cANCA is associated with granulomatosis with polyangiitis (Wegener’s) affecting lungs and kidney; whilst pANCA is associated with glomerular nephritis ( U&Es). Both types can be associated with ankylosing spondylitis (AS).
U&Es). Both types can be associated with ankylosing spondylitis (AS).
Clinical symptoms will drive some of the decision-making in terms of requesting and interpreting autoimmune blood tests. For example, a patient with AS will usually have a different presentation from one with RA. As discussed in Chapter 4, these patients may already have outlying values for WBC, CRP and PV because of their underlying condition. As the condition flares, these changes may be significant but nevertheless clinically expected given the condition. However, we still need to be aware that another new condition (such as a bacterial infection) could also modulate WBC, CRP and PV, so we should question baseline changes and symptoms.
Typical autoimmune profiles
A typical systemic lupus erythematosus (SLE) blood profile could be that about 95% of patients with SLE have a positive ANA. SLE is often seen with thrombocytopenia (low platelets) and high levels of anti-single-stranded DNA Ab (a type of antibody usually found in these conditions, usually requested by a consultant).
A typical RA blood profile could be that about 80% of patients are positive for RF and negative for HLAb27. This often occurs with raised neutrophils and WBC, raised CRP, raised PV and raised globulin.
A typical AS blood profile could be that about 80% of patients are positive for HLAb27 and negative for RF. If a patient is HLAb27 negative then we could consider two new genetic tests: Type 1 tumour necrosis factor receptor shedding aminopeptidase regulator (ARTS1) and interleukin 23 receptor (IL23R). This often occurs with raised neutrophils, WBC, CRP and erythrocyte sedimentation rate (ESR).
Polymyalgia rheumatica (PMR) means ‘pain in many muscles’ and is thought to be mainly due to inflammation of the muscle’s vascular system. A typical PMR blood profile could be raised ESR and CRP. These patients are usually negative to rheumatoid factor (RF) but positive to HLAb27, and some have elevated platelets and low RBC (although the reason is unclear). If the patient is on certain types of statins, measuring total creatine kinase (CK) may help identify muscle damage. CK is a muscle enzyme and its value in the blood increases in relation to muscle damage. It is thought that some statins can induce muscle damage and cause pain.
Polymyositis is the presentation of muscle antigen as foreign material. A typical blood profile could be positive for ANA and then positive for the Anti Jo subset (a type of antibody usually found in these conditions). These patients could also have raised serum creatinine kinase (CK), and usually raised CRP, PV and ESR.
Reactive arthritis is often linked to an underlying viral or bacterial infection that has induced an immune response and is not subsequently ‘switched off’. A typical blood profile could be positive for HLAb27 and negative for RF, with raised CRP and ESR.
Psoriatic arthritis (PA) causes connective and musculo-skeletal damage, which is usually linked to prolonged psoriasis. Psoriasis is the autoimmune destruction of the skin, and a typical PA profile could be negative for RF but positive for HLAb27, with raised CRP and ESR.
Myeloma
A myeloma is a cancer of the B cell lymphocytes. Often, damaged cells aggregate in the bone ( bone pain, bone profile test and raised calcium (Ca)). The cells often produce a monoclonal globulin protein called a Bence Jones protein. The types of globulins produced by the B cells can be further assessed by means of electrophoresis, which can help differentiate between different types of myeloma and leukaemia. This gives profiles of gamma, IgG, IgM and IgD and so on. The patient will often also have raised WBC (more B cells), raised globulin (from Ab production) and raised PV due to more ‘stuff’ (globulins and B cells) in the blood and raised ESR.
bone pain, bone profile test and raised calcium (Ca)). The cells often produce a monoclonal globulin protein called a Bence Jones protein. The types of globulins produced by the B cells can be further assessed by means of electrophoresis, which can help differentiate between different types of myeloma and leukaemia. This gives profiles of gamma, IgG, IgM and IgD and so on. The patient will often also have raised WBC (more B cells), raised globulin (from Ab production) and raised PV due to more ‘stuff’ (globulins and B cells) in the blood and raised ESR.
The correct and normal antibody produced by the B cell has two major components – a heavy chain and a light chain. In some myeloma patients, the faulty B cell produces only the light chain and this is called the Free Light Chain (or FLC or paraprotein or, when measured in the urine, Bence Jones Protein). Take care here, as someone with chronic kidney disease may present with an artificially raised FLC but have no myeloma (their kidney hasn’t got rid of the small amount of normal FLCs we make each day). We don’t know exactly why this is the case.
Storytelling: Imagine a B cell called Bob. Bob makes a certain type of normal antibody. The clever part is that, once Bob dies, Bob’s children will also only ever make the same antibody, and the grand-kids and the great-grandchildren likewise as they are all clones of the original Bob. Imagine we also have B cells called Brenda, Bruno, Bill, Bella, Beatrice, Bellatrix, Bethan and Bomber. Each of these B cells produces a different antibody so we have ‘polyclonal’ antibody production. All their clones will continue to produce these different antibodies. But if the bone marrow goes wrong and only makes Bobs, then we may switch from a ‘polyclonal’ profile to a ‘monoclonal’ profile, as only one type of B cell is being produced.
Fibromyalgia/Chronic fatigue syndrome (CFS)
Fibromyalgia is an example of a condition that significantly affects millions of people and yet we have no single blood test to diagnose fibromyalgic conditions or conditions such as CFS. The current approach is to exclude symptomatic presentation by checking for infection, anaemia, thyroid symptoms, etc., as well as clinical history. The main reason why we have no blood test is due to the likely pathology being the disruption in a neurotransmitter such as substance P, cytokines or chemokines produced by inflammation and the way in which the muscle and nerves talk to the brain. A chemical change is happening but, at present, a simple, cost-effective, reliable test hasn’t been identified. Once we have a reliable means of diagnosis, the next challenge will be to find a reliable treatment.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


