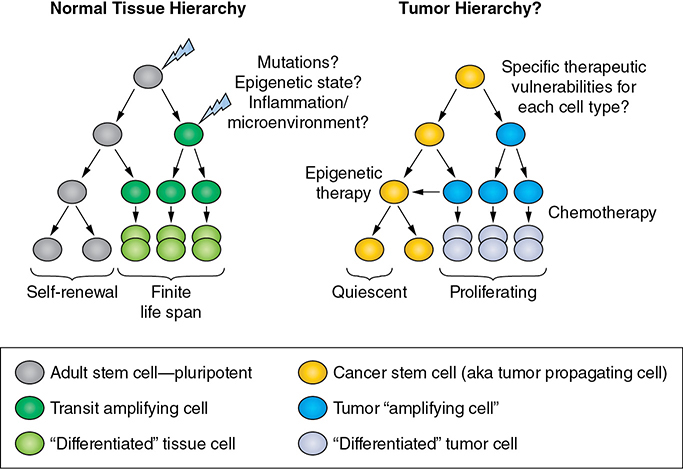
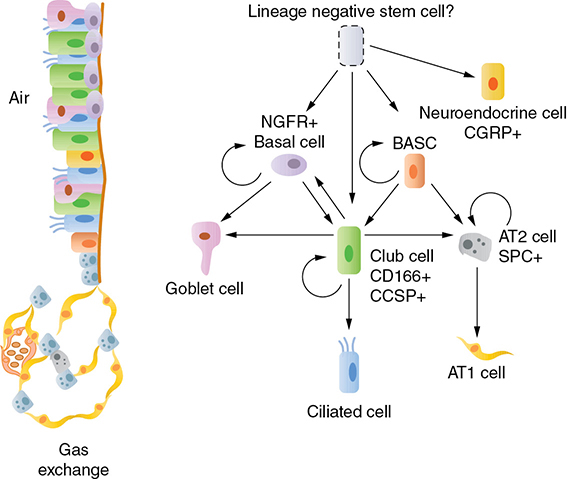
A 50-year-old heavy smoker was treated for small cell lung cancer, limited stage, with chemotherapy and radiation. The bulky tumor in his chest was no longer seen after the treatment, and he was told he had a complete response. Two months following the treatment, the cancer recurred and was resistant to any further systemic therapy. He asks during his last clinic visit before going to hospice, “How did the cancer come back so quickly, and why was it not cured when I had a complete response?” Learning Objectives: 1. What is meant by the term cancer stem cells? 2. How can cancer stem cells (CSCs) explain treatment resistance and recurrence of disease? 3. What are the normal stem cells in the lung that the CSCs may be mimicking? Lung cancer is a progressive disease arising from accumulation of genetic mutations and natural selection of the genetic clones most fit to continue proliferation. However, even within isogenic cancer cell populations, heterogeneity in phenotypes exists. For example, not every lung cancer cell can grow ex vivo in two-dimensional or three-dimensional culture,1,2 and it does not appear that every cell has an equal ability to survive chemotherapy, evade the immune system, or metastasize.3,4 As early as 1858, the idea of “stemness” in cancer was raised by the pathologist Rudolph Virchow,5 and throughout the past century the idea that tumors are driven by a population of stem-like cells has been constantly proposed as the reason for clonal tumor cell heterogeneity. In the past several decades, the idea has been formally termed the cancer stem cell hypothesis.6,7 The CSC hypothesis proposes that tumors can be hierarchically organized, and that only the cancer cells at the top of the hierarchy have the unique properties of self-renewal and the ability to differentiate into multiple lineages (Figure 8-1). In normal tissues, these traits of self-renewal and differentiation allow stem cells to repopulate organs during homeostatic turnover and after tissue injury. In the context of cancer, “stemness” implies that these cancer cells have a more unlimited proliferative potential than “nonstem” cancer cells and therefore that they are the cells able to drive tumor growth long term. Corollaries to the CSC hypothesis include that CSCs are relatively resistant to chemotherapies through multiple mechanisms, including relative quiescence; that CSCs drive recurrent disease; and that CSCs are responsible for seeding metastases.3,4,8 Whether one or all of these properties of long-term tumor growth, disease resistance to therapy, and metastatic spread of cancer can be attributed to a single subpopulation of cancer cells relies largely on the composition of the tumor, including the mutations present, the polyclonality of the tumor, and the differentiation state of the cells within the tumor.8 In order to fully appreciate the possible traits of a CSC population, it is first necessary to understand the traits of the normal epithelial differentiation hierarchies that the tumor cells could be mimicking. Figure 8-1. Parallels between normal tissue hierarchy and tumor cell hierarchy. Whether cancer stem cells (CSCs) exist within a tumor population depends on extrinsic cues such as inflammation and the microenvironment, as well as cell intrinsic properties. The cell intrinsic properties include the epigenetic state of the cell that acquired sufficient mutations to become malignant and the specific pathways of the mutations. Understanding both the normal lung epithelial hierarchies and hierarchies that exist within the distinct subtypes of lung cancer holds promise to define specific vulnerabilities of both genetic and epigenetic states for lung cancers. In this chapter, the reader will learn about the diverse epithelial cell types from which lung tumors can arise and how tumor cell characteristics may resemble the normal epithelial hierarchies found in lung. Understanding these hierarchies is key to exploring the CSC hypothesis in lung cancer, which posits that a rare stem-like population of cells drives tumor growth and recurrence. The reader will learn about possible CSC markers for various subtypes of lung cancer and learn about efforts in the field to target CSCs. Several distinct stem/progenitor cell pools have been identified in the lung, including basal cells, club cell progenitors, alveolar cell progenitors, and bronchioalveolar stem cells9–12 (Figure 8-2). Each of these cell types has some capacity to self-renew and to give rise to other lineages of lung epithelial cells in the contexts of tissue injury and homeostatic turnover. In experimental models, non–small cell lung cancer may arise from any of these stem/progenitor pools, and perhaps other uncharacterized “lineage-negative” cell populations, dependent on the genetic perturbations used.13–17 As we learn more about the diverse cell types that have regenerative capacity in the adult lung, we will undoubtedly uncover corresponding molecular cell types of non–small cell lung cancer that recapitulate distinct cellular hierarchies. It is important to remember that due to microenvironmental changes and genetic mutations, CSCs within a tumor may not still resemble the cell from which they arose, but rather may resemble a cell upstream or downstream in the hierarchy due to epigenetic reprogramming. Figure 8-2. Normal progenitor cell pools for cancer stem cells. Numerous distinct cell types exist within the normal lung epithelium. The cells with self-renewal capacity include basal cells of the trachea and upper bronchi that express NGFR and KRT5; secretory club cells that express CD166 and CCSP; and alveolar type II cells that express SPC. Also within the bronchiolar epithelium are innervated CGRP+ neuroendocrine cells, mucus-producing goblet cells, and multiciliated cells. In the murine lung, at the bronchioalveolar duct junction, a cell type that can give rise to both bronchiolar and alveolar lineages is termed the bronchioalveolar stem cell (BASC). Alveolar type I cells are thin cells that perform gas exchange in the distal lung. Each of these cell types has a distinct epigenetic state, and in theory any of these cells can serve as the cell of origin for lung cancer if the proper genetic mutations are accumulated. Many recent reports have suggested a lineage-negative lung epithelial cell may be the most primitive lung cell with the greatest differentiation potential, although further characterization of this elusive cell type is needed. The two major subtypes of non–small cell lung cancer are adenocarcinoma and squamous cell carcinoma. Historically, these two major subtypes have been hypothesized to arise from distinct cell populations within the lung due to differences in anatomical location and marker expression retained in the cancers. Adenocarcinomas tend to arise in the more distal airspace and have markers consistent with distal lung cell origin, including proteins expressed by alveolar type II cells such as the homeobox transcription factor NK2 homeobox 1 (NKX2-1) and surfactant protein C (SPC). Some adenocarcinomas are more “bronchiolar” in phenotype and therefore express markers that secretory club cells of the airways express, including club cell secretory protein (CCSP) and the transcription factor SOX2. Supporting the idea that CSCs in adenocarcinoma may be in a more bronchiolar state, CD166 (also known as ALCAM) has been shown to mark CSCs in both adenocarcinoma and squamous cell carcinoma xenografts and was shown to enrich for the club cell lineage from human tracheal cell preparations.18,19 Squamous cell carcinomas tend to arise more proximally, sometimes even connecting physically to the pseudostratified epithelium of the upper airway. However, mixed adenosquamous tumors and peripheral squamous tumors exist in patients as well as in mouse models, and these observations suggest that squamous cell carcinomas can arise from adenocarcinomas or alveolar cells given the correct microenvironment and genetic alterations. Regardless of their genesis, squamous cell carcinomas express markers consistent with basal cells, which are the stem cells of the trachea and upper bronchi, including KRT5, TP63, and NGFR9,18; therefore, it is possible that CSCs within these tumors also have basal cell-like characteristics. Indeed, an NGFR+ cell population was found to have CSC potential by serial orthotopic injections in a mouse model of lung squamous cell carcinoma.20 In addition to the lineage markers described, many groups have focused on the known putative CSC markers, including CD133 (prominin), ALDH1 (aldehyde dehydrogenase), and CD44. CD133 was significantly associated with disease recurrence, resistance to therapy, and decreased overall survival.21,22 ALDH1 also had some prognostic value, being associated with decreased survival, most specifically in the adenocarcinoma subtype.21 Using primary human lung cancer xenografts, sphere cultures, and established cell lines, several groups have demonstrated that CD133 is a marker of functional CSCs with the ability to seed tumors in vivo and survive chemotherapy.21 Studies of ALDH1 expression in combination with CD133 or CD44 have shown that ALDH1+ cells have an increased ability to seed tumors in serial transplantation assays when compared to the bulk or ALDH1- cells, strongly indicating that cells with these markers could be bona fide adenocarcinoma CSCs.21,23 Importantly, many of these studies demonstrated that the cells with functional CSC properties also expressed high levels of NOTCH proteins.21,22 As described in material that follows, NOTCH inhibition could be a vulnerability for non–small cell lung cancers. Due to limitations of primary human tissues, including large interpatient heterogeneity and small sample size, much of what we understand about functional CSCs has been learned in genetically engineered mouse models (GEMMs) of lung cancer. GEMMs representing adenocarcinoma, squamous cell carcinoma, and mixed adenosquamous cancer have been established, and new genetic combinations are consistently being produced and assessed for phenotype.24 Using the mouse adenocarcinoma model driven by oncogenic KRAS and loss of Tp53, a population of tumor cells highly enriched for tumorigenic potential was identified to be CD24+/INTGA6+/NOTCH3+; similarly, a population of highly metastatic cells was identified to be CD24+/SCA1+.25,26 In a mouse model of squamous cell carcinoma driven by biallelic deletion of LKB1 (STK11) and PTEN, the CSC phenotype was SCA1+/NGFR+, and the CSCs were enriched for expression of the immune-evasion marker PD-L1.20 As new genetic combinations are tried, it will be very important to compare CSC phenotypes between models, given that a direct comparison of one stem cell marker, SCA1, in several GEMMs demonstrated that CSCs can differ greatly in phenotype dependent on genotype.27 Therefore, going forward the field must start to acknowledge both molecular subtype and genotypes as drivers of CSC phenotypes, and mouse models are an excellent way to control for tumor genotype and produce enough tissue to thoroughly test the CSC hypothesis. Due to the heterogeneity of the disease, targeting CSC populations in non–small cell lung cancer will likely require many approaches. Targeting metabolic programs in CSCs, the ability of CSCs to evade the immune system, and the epigenetic state of CSCs addresses viable approaches to prevent disease recurrence that are currently being heavily explored for non–small cell lung cancers. In terms of targeting a signaling protein that CSCs rely on, one promising target that has been validated in several systems is NOTCH3 for lung adenocarcinomas. However, there is not yet a NOTCH3-specific inhibitor, and it is unclear if gamma-secretase inhibition, which targets all forms of NOTCH, would be useful. NOTCH1- and NOTCH2-inactivating mutations are found in both lung squamous cell carcinoma and small cell lung cancer, so it is conceivable that inhibition of all NOTCH receptors would both target the adenocarcinoma CSC pools through NOTCH3 and drive the tumor to “transdifferentiate” to a more squamous or neuroendocrine fate through inhibition of NOTCH1 and NOTCH2. More research on this pathway could allow for a more specific inhibitor that targets only NOTCH3 to be developed. Targeting epigenetic programs also holds some promise for the field. For example, it was recently identified that inhibition or knockdown of the histone methyltransferases G9A or GLP allows for an expansion of the metastatic CSC pool in KRAS-driven cancers.28 Therefore, one method to target the CSC pool could be through inhibiting histone d-methylases, which was tested pharmacologically with the inhibitor JIB-01.28 Inhibition of JIB-01 during establishment of taxane-resistant non–small cell lung cancers was also effective,29 suggesting that histone demethylase inhibition may be one way forward in lung adenocarcinomas. In the case of small cell lung cancer, it is clear that tumors comprise cells that are neuroendocrine in phenotype. This phenotype is robust and can be validated by several markers specific to the pulmonary neuroendocrine lineage of the lung epithelium, including calcitonin gene-related peptide (CGRP), chromogranin A, and neuron-specific enolase. In the normal lung, neuroendocrine cells reside anatomically at features termed neuroendocrine bodies, which are enervated groups of cells within the bronchiolar epithelium. Study of the genesis of these neuroendocrine bodies in developing lung has suggested that the embryonic alveolar lineage can give rise to these neuroendocrine bodies.30 This possible lineage relationship between alveolar cells and neuroendocrine cells is further supported by the clinical observation that EGFR-driven lung adenocarcinomas, which typically resemble alveolar type II cells, can transdifferentiate into small cell lung during acquired resistance to EGFR tyrosine kinase inhibitors and can return back to the adenocarcinoma fate after the tyrosine kinase inhibitor is removed.31 However, studies in the adult mouse have suggested that although neuroendocrine cells can serve as progenitor cells to repopulate the club cell lineage,30,32
8
THE CANCER STEM CELL HYPOTHESIS OF LUNG CANCER
NON–SMALL CELL LUNG CANCER STEM CELLS
TARGETING CANCER STEM CELLS IN NON–SMALL CELL LUNG CANCER
SMALL CELL LUNG CANCER STEM CELLS
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


