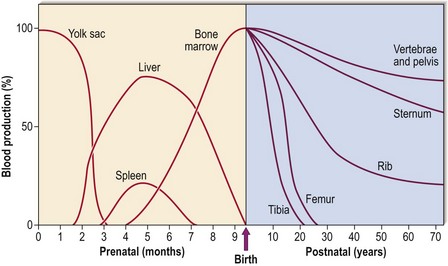
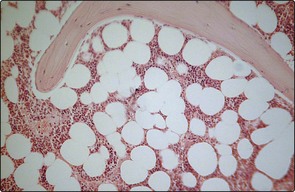
1 In early fetal life, blood is produced in the mesoderm of the yolk sac. During the second to seventh months the liver and spleen take over. Only in the last 2 months of fetal development does the bone marrow become the predominant site of blood formation. During childhood, marrow in the more peripheral bones becomes gradually replaced by fat, so that in adult life over 70% is located in the pelvis, vertebrae and sternum (Fig 1.1). This explains the sites used for bone marrow sampling (see p. 106). A trephine biopsy allows a two-dimensional view of the bone marrow down the light microscope (Fig 1.2). Haematopoietic cells of varying lineage and maturity are packed between fat spaces and bony trabeculae. Ultrastructural studies reveal clusters of haematopoietic cells surrounding vascular sinuses which allow eventual discharge of mature cells into the blood. Different lineages are compartmentalised; for example, the most immature myeloid precursors lie deep in the marrow parenchyma while more mature forms migrate towards the sinus wall. Lymphocytes tend to surround small radial arteries while erythrocytes form islands around the sinus walls.
The bone marrow
The structure of the bone marrow
Oncohema Key
Fastest Oncology & Hematology Insight Engine