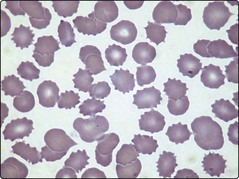
48 Diseases of the kidney are associated with a remarkably wide range of possible haematological abnormalities (Table 48.1). Table 48.1 Haematological changes in renal disease 1The complex coagulation abnormalities of renal failure usually lead to a bleeding tendency but nephrotic syndrome is associated with an increased incidence of thrombosis. Anaemia is almost inevitable in chronic renal failure. The pathogenesis is complex but impaired erythropoietin production is the principal cause. Other possible contributory factors include the release of inhibitors of erythropoiesis, mild haemolysis and iron deficiency. The anaemia of renal failure is typically normocytic and normochromic. A characteristic finding in the blood film is the presence of burr cells (Fig 48.1). The best treatment of anaemia is resolution of the underlying renal problem (e.g. by transplantation), but where this is not feasible, recombinant erythropoietin is the treatment of choice. Intermittent bolus administration generally leads to a marked improvement in anaemia and transfusion independence. A failure of the anaemia to respond to erythropoietin should prompt a search for other aetiologies such as iron deficiency. Paradoxically, some forms of renal disease can lead to increased red cell production and clinical polycythaemia (see Table 48.1). This arises either from inappropriate secretion of erythropoietin by a kidney tumour or from local renal hypoxia promoting erythropoietin release from normal cells. Polycythaemia can be the presenting feature of renal carcinoma and rapid identification of the malignancy may allow curative surgical treatment. Benign diseases such as polycystic disease and hydronephrosis probably cause polycythaemia by inducing renal ischaemia. The polycythaemia of renal disease is not an appropriate physiological response and patients with high haematocrits can derive benefit from regular venesection. Chronic renal failure is also associated with a large number of possible platelet and coagulation abnormalities. The increased risk of bleeding in these patients is generally caused by the complex interaction of abnormalities shown in Table 48.1. Anaemia tends to worsen bleeding by interfering with the normal interaction between platelets and vascular endothelium.
Systemic disease
Renal disease
Abnormality
Clinical association
Red cells
Anaemia
Chronic renal failure
Polycythaemia
Renal carcinoma, cystic disease, hydronephrosis, parenchymal disease, Bartter’s syndrome, renal transplantation
Burr cells
Renal failure
Haemostasis
Abnormal platelet function
Renal failure
Thrombocytopenia
Disordered coagulation1
Oncohema Key
Fastest Oncology & Hematology Insight Engine