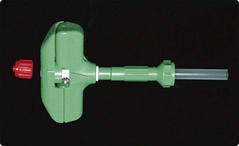
53 The patient lies in the left or right lateral position and the skin over the posterior iliac crest is cleaned with antiseptic prior to screening with sterile drapes. The crucial next stage is to properly identify the bony landmarks (Fig 53.1). This is straightforward in most patients but can be problematic in obese subjects. If there are real difficulties in locating the posterior iliac crest then the anterior crest or the sternum may be considered or the procedure may be performed under CT guidance. A local anaesthetic is infiltrated into the skin and then down to the periosteum. Before use it should be checked that the marrow aspirate needle stylet is easily withdrawn and the guard is removed (this is only required for sternal aspirates). The needle (Fig 53.2) is inserted through the skin and subcutaneous tissues at the site of local anaesthetic infiltration until the periosteum is encountered. It is pushed through the periosteum with a deliberate screwing motion (alternating clockwise and anti-clockwise) – a ‘give’ is felt as the marrow cavity is entered. The stylet is withdrawn and a syringe attached to the needle (Fig 53.3). Approximately 0.5 mL of marrow is aspirated into the syringe. The patient should be warned that this stage often causes pain but that it is momentary. Fig 53.1 Anatomy of the posterior iliac crest.
Bone marrow aspiration and trephine biopsy
Bone marrow aspiration
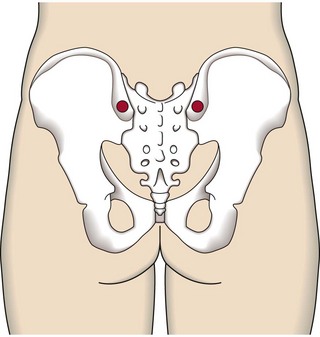
Possible sites for marrow sampling are indicated in red.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oncohema Key
Fastest Oncology & Hematology Insight Engine