Options for surgical treatment of early larynx cancer include open conservation laryngeal surgery (CLS) or transoral endoscopic resection, with either traditional “cold-steel” phonosurgery or transoral laser microsurgery (TLM). Although the use of open techniques has declined, the emergence of transoral endoscopic head and neck surgery (eHNS)1 has rekindled interest in functional organ-preservation surgery of the larynx and has expanded the available multidisciplinary treatment options for patients. Chen et al.2 recently found that among patients with early-stage cancer, those receiving primary surgery increased (from 20% in 1985 to 33% in 2007), whereas the use of RT decreased from 64% to 52%. However, for intermediate- and advanced-staged cancers, Hoffman described the opposite trend: a greater role for radiation and concurrent chemoradiation over these same decades.3 This review of the National Cancer Database between the years 1985 and 2001 found a trend toward decreasing survival among patients with laryngeal cancer from the mid-1980s to mid-1990s. During these decades, the authors found a significant increase in chemoradiation, with a concomitant decline for the role of surgery.
Over this same time period, there has been a sea change within the field of head and neck surgery. For years, cancer surgery for tumors of the larynx has been synonymous with “total laryngectomy.” However, now an array of new surgical approaches, including transoral minimally invasive surgery of the larynx, and supracricoid partial laryngectomy (SCPL) offer the potential to improve clinical outcomes, function, and quality of life.4 Since these techniques are just now being routinely accepted and employed within the multidisciplinary paradigm, we review here the current role of surgery for patients with laryngeal cancer.
ENDOSCOPIC RESECTION
Vocal Stripping, Cold-Steel Resection, and Phonosurgery
Vocal cord stripping may still occasionally be performed for selected superficial, noninvasive lesions of the glottis.5,6 In general, this previously accepted technique of vocal cord stripping has fallen out of favor due to the poor voice results that often accompanied these procedures. Early malignant tumors, and even extensive premalignant disease, may seem superficially invasive, by preoperative exam in the clinic, but in fact often have invasion of the vocal ligament.7 Our improved understanding of the layered vocal fold from Hirano8 and the refinement of microflap techniques have pushed this technique toward obsolescence. The stripping technique is rather imprecise in peeling away the epithelium in the layer of the superficial lamina propria. Failure to preserve this layer when possible, and in a nonuniform manner, has relegated its use to a vocal fold scar model for investigational studies. The more precise technique of microflap excision has proven to be voice preserving in many instances and successful in the treatment of precancerous lesions. Ossoff’s work detailed the successful regression of preneoplastic lesions with serial microflap excision of dysplasia.9
Technique. Rigid laryngoscopy in suspension under microscopic guidance is used for resection. Microlaryngeal instrumentation is used to sharply excise the tumor from the vocal folds. In the microflap technique, an incision is made lateral to the lesion, which is bluntly undermined and then sharply excised.
Transoral Laser Microsurgery
In contrast to transoral cold-steel “phonosurgery,” the concept of TLM encompasses the laser-based surgical resection of tumors of the larynx through the mouth. For the purposes of this chapter, we will limit this terminology to TLM of the larynx, but the technique can easily and reliably be applied to the oral cavity, oropharynx, and hypopharynx as well. TLM as a surgical approach is founded upon the historical evolution of the field of otolaryngology and reflects the practitioner’s ability to look through the transoral window into the laryngopharynx and treat myriad conditions. Traditionally, TLM is done using a line-of-sight laser beam aided by a microscope. As the use of the operating microscope with the laser greatly facilitated complete tumor excision that was not possible with cold surgical techniques, advances in technology will likely continue to expand the repertoire of the TLM approach. With continued advances in lasers, robotics, and visualization technologies, TLM techniques will continue to evolve and improve.
In 1972, Jako and Strong published the first clinical experience using the carbon dioxide laser as part of transoral microsurgery for the treatment of benign and early malignant lesions of the larynx.10 The technique was widely adopted among laryngologists, but failed to take hold within head and neck surgery. Steiner11,12 and others in Europe developed this technique and made critical conceptual advances and improvements in instrumentation. Since then, TLM has played a much greater role within the multidisciplinary paradigm, and its use has been expanded for tumors throughout the upper aerodigestive tract and for more advanced-stage tumors.12
TLM may or may not entail a “piecemeal excision” of the laryngeal tumor. Small lesions can be removed en bloc or by dividing the tumor across its main axis. Although this approach violates Halstedian technique, advocates argue that by appreciating the unseen depth of the lesion, especially near critical and/or unique anatomy, an adequate oncologic resection can be achieved, while minimizing the sacrifice of surrounding normal structures. Using the operating room microscope, which provides magnification of 4× to 12×, the endoscopic surgeon can have significantly improved visualization and thus more detailed understanding of the interface between tumor and normal tissue.13,14 By dividing the tumor, though, the surgeon must bear additional responsibility to provide adequate margins through close coordination with pathology—as well as close tumor surveillance postoperatively. In fact, in the largest series published on the role of margins in TLM, Jackel et al.15 found that 30% of patients required some additional surgery for a variety of T1 to T4 tumors treated with TLM, mostly for inadequate margins on final histopathology, despite negative frozen sections. Most of these patients (82% of the re-resected specimens demonstrated no evidence of residual tumor) had similar rates of local control as those patients in whom revision was not necessary. This discordance suggests the inherent challenges associated with TLM and underscores close partnership with the surgical pathologist. However, patients with residual tumor after revision TLM showed a significant reduction in locoregional control as well as larynx preservation. However, in this study, overall survival was not significantly affected15; rather, there is a need for open surgery and salvage radiation therapy for these patients with positive re-resection margins.
Despite these concerns, TLM has outcomes comparable to open conservation surgery and radiation therapy for patients with T1 to T2 glottic cancer. Local control for T1 lesions was 77% to 92% and that for T2 tumors was 61% to 88%. After salvage therapy, an “ultimate” local control rate was well above 90% with 5-year disease-specific survival of 86% to 98%.16,17,18,19,20,21,22 Authors quote high rates of overall larynx preservation, when TLM is selected as the first treatment modality with rates ranging from 90% to 99%,16,17,18,19,21,22 although one group reported a larynx- preservation rate of 97% for T1 tumors and 82.5% for T2 lesions.20 Critics of TLM point out that most of the literature is derived from single institutional retrospective reviews. However, there remains no NCI, or industry-funded cooperative group, or funding to support central data collection and prospective investigation.
Despite these current roadblocks to prospective clinical investigation, Hinni and his colleagues assembled in 2007 a multidisciplinary review of TLM in the treatment of advanced laryngeal cancer of stages T2 to T4. Two-year larynx preservation and local disease control rates were 92% and 82%, respectively. Five-year Kaplan-Meier estimates of overall survival were 55%, in keeping with results from the RTOG-911. A number of larger series such as this and other now appear to suggest that TLM for the treatment of larynx cancer has local control rates, and larynx preservation, on par with open approaches with better functional outcomes, and in properly selected patients on par with radiation therapy.
First and foremost, TLM represents a dramatic break from traditional compartmental or subunit surgery for the resection of laryngeal tumors. Yet this “precision medicine”23 approach using transoral eHNS creates challenges in nomenclature and description of the TLM procedure performed. In this new approach, each endoscopic resection is personalized for the individual patient’s tumor and is thus not removed in the traditional whole organ or compartmental fashion. In 2000, Remacle led the European Laryngological Society (ELS) effort to develop a classification system for the endoscopic resection of glottic cancer.24 In this schema, endoscopic cordectomy is categorized into five types, ranging from subepithelial to anterior commissurectomy with bilateral anterior cordectomy, to “extended cordectomy,” representing the full array of partial laryngectomies24,25 (Table 18.15). In 2009, the ELS proposed a classification system for endoscopic supraglottic laryngectomy with four categories, ranging from limited excision to a lateral supraglottic laryngectomy26 (Table 18.16).
Although TLM offers many advantages to the surgeon, there are also important limitations. First, not every patient may be a suitable candidate. Inadequate endoscopic exposure due to dental occlusal, deformity, retro- or micrognathia, or macroglossia may limit the number of patients eligible for endoscopic resection. Second, adverse tumor features, such as an endophytic growth pattern, perineural invasion, or occult extralaryngeal spread,27,28 are associated with poor oncologic and functional outcomes. Previous radiation treatment may also be a relative contraindication. Although TLM may be effective in this setting, identification of tumor margins and prolonged mucosal healing are more difficult during endoscopic resection after radiation therapy.
Steiner et al.29 reported on 34 patients with early- or advanced-stage recurrent glottic carcinoma after radiation therapy. Twenty-four patients (71%) were cured after one or more TLM. Patients with early-staged recurrent carcinomas had lower rates of local recurrences and salvage total laryngectomy than did patients with advanced recurrent cancers. However, in this experience, more than half of the patients required at least two TLM procedures to achieve disease control, underscoring the difficulty of this approach. Similarly, Quer et al. presented a series of patients treated with TLM for both supraglottic and glottic cancers, recurrent after radiation.30 Although disease-free survival rate after 5 years was 100%, multiple procedures were required to achieve disease control. For these reasons, the role of TLM in the setting of surgical salvage after radiation should be carefully considered. For small limited recurrences (rT1), TLM may appear to offer good results. For more extensive recurrence after radiation, open surgery may be a better option. What is clear, though, is that TLM has its best role to play as primary, rather than salvage, therapy.
TABLE 18.15 Schema for Endoscopic Cordectomy
I
Subepithelial cordectomy
II
Subligamental cordectomy
III
Transmuscular cordectomy
IV
Total cordectomy
V
Extended cordectomy
Va including contralateral vocal fold
Vb including the arytenoids
Vc including the ventricular fold
Vd including the subglottis
VI
Anterior commissurectomy with bilateral anterior cordectomy25
Source: From Remacle M, Eckel HE, Antonelli A, et al. Endoscopic cordectomy. A proposal for a classification by the Working Committee, European Laryngological Society. Eur Arch Otorhinolaryngol. 2000;257:227-231, with permission.
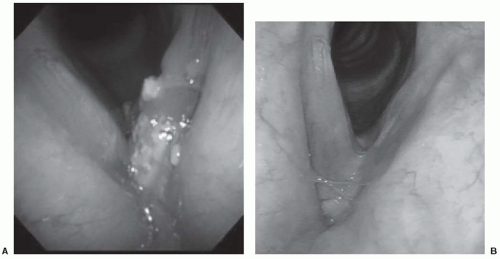
As primary treatment for laryngeal cancer, TLM is associated with several advantages in the short-term benefits (Fig. 18-28A,B). Tracheotomy is rarely needed. Swallowing dysfunction is rare, especially for patient undergoing endoscopic resection for glottic cancer. These functional advantages are also associated with shorter hospital stays and lower costs of treatment.31 In most cases, endoscopic surgery broadens the management possibilities for persistent or recurrent disease; salvage for failure after TLMs can be approached with further endoscopic, or open surgery, or with radiotherapy.5,14
TABLE 18.16 Classification of Endoscopic Supraglottic Laryngectomy
I
Excision of small, superficial lesions confined to single subsite of the supraglottis
II
Medial supraglottic laryngectomy with preservation of the preepiglottic space
IIa with superior hemi-epiglottectomy
IIb with total epiglottectomy
III
Medical supraglottic laryngectomy including the preepiglottic space
IIIa with preservation of the ventricular fold
IIIb with resection of the ventricular fold
IV
Lateral supraglottic laryngectomy
IVa with resection of the ventricular fold
IVa with resection of the arytenoid
Source: From Remacle M, Hantzakos A, Eckel H, et al. 1, 2. Endoscopic supraglottic laryngectomy. A proposal for a classification by the working committee on nomenclature, European Laryngological Society. Eur Arch Otorhinolaryngol. 2009;266:993-998, with permission.
FIGURE 18-28. Transoral laser microsurgery for glottic laryngeal cancer. A: Preoperative laryngoscopy demonstrates a tumor of the left transglottic larynx in a 63-year-old male smoker with T2N0M0 squamous cell carcinoma. The tumor extends from the false cord to the subglottis. B: Postoperative view at 24 months.
Technique. Using suspension direct microlarynoscopy, the carbon dioxide laser is used to transect the tumor to determine the depth of invasion. Using microlaryngeal instrumentation, it is then typically resected, either en bloc, or in the fashion proposed by Steiner,32 maintaining orientation of the specimens removed in order to evaluate for margin status. The technique usually varies from traditional open CLS in following the tumor, rather than subscribing to the compartment resection theory of the larynx. Healing is by secondary intention, with contraction of the resected tissue, avoiding the need for reconstruction (Fig. 18-29).
Conservation Laryngeal Surgery
CLS33 represents a broad array of open surgical techniques, ranging from laryngofissure with cordectomy to supracricoid laryngectomy. In addition to achieving comparable rates of local control, with CLS, surgeons can achieve functional organ preservation by understanding the cricoarytenoid unit34 (defined as arytenoid, cricoid cartilage, associated muscles, and corresponding innervation by the superior and recurrent laryngeal nerves) as the basic functional unit of the larynx, not the vocal cord alone.33
Rarely, laryngofissure with cordectomy may still be required, perhaps for patients with poor transoral exposure. The thyroid cartilage is divided to gain access to the endolarynx, and with wide visualization, the tumor is excised. Historically, postoperative tracheotomy was always required,35 but Laccourreye et al. described a series of 33 patients where this was not needed: local control was 100%; 5-year survival rate 97%.36
Vertical partial laryngectomy (VPL), also known as hemilaryngectomy, is a time-honored approach to resecting an entire ipsilateral glottic larynx, including paraglottic space and corresponding thyroid ala, but preserving the ipsilateral arytenoid. Local control rates for T1 cancers range from 89% to 100%.37,38,39,40 Involvement of the anterior commissure decreases local control; one study reported that anterior commissure involvement decreased local control from 93% to 75%. For tumors involving the anterior commissure or the anterior-most aspect of the contralateral vocal fold, an extended VPL or frontolateral vertical hemilaryngectomy can be done. Yet for larger T2 tumors, VPL may be less effective, with local control rates of 74% to 86%.37-39,41 Ultimately, for preoperative decision making, T classification may be less effective than careful laryngoscopic exam: for instance, patients with significant extension to the subglottis or supraglottis, or without impaired vocal cord mobility may fare worse.
Only gold members can continue reading. Log In or Register to continue