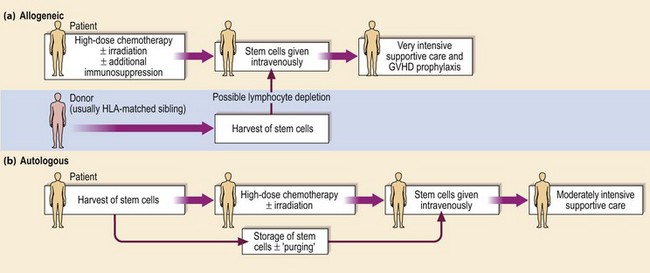
28 The allogeneic procedure is outlined in Figure 28.1. The patient’s own haematopoietic stem cells, immune system and residual tumour cells are conventionally destroyed by conditioning treatment with high-dose chemotherapy and (usually) radiotherapy prior to intravenous infusion of stem cells harvested from the healthy donor. The ideal patient has a disease curable by allogeneic SCT but not by less toxic treatment and is young (less than 40 years old). The ideal donor, excepting the rare presence of a twin, is a sibling genotypically matched with the recipient for HLA-A, B and DR. The genes for HLA are found on chromosome 6 and so inheritance follows the rules of simple Mendelian inheritance; two siblings have a one in four chance of sharing the same two HLA haplotypes. With relatively small family size in the Western world, only around 30% of patients will have an HLA-identical sibling. Transplants from HLA-haploidentical relatives have been associated with a high rate of morbidity and mortality. An alternative strategy is to search for an unrelated volunteer donor who is a phenotypic HLA match. From the worldwide databases of 18 million HLA-typed volunteers, around 50% of Caucasian patients can be found a suitable donor. Success rates are lower in other ethnic groups. Use of a HLA-mismatched donor leads to an increase in the incidence and severity of the adverse effects of SCT. Weaker transplant reactions result from mismatch for minor histocompatibility antigens, single peptides derived from polymorphic proteins which may differ between donor and recipient. After conditioning treatment there is a period of about 3 weeks before ‘engraftment’ during which the patient is severely pancytopenic and immunosuppressed and requires intensive supportive care with blood products and aggressive treatment of any infection. Major adverse events include graft failure with rejection arising from a failure to immunosuppress the patient adequately, and graft-versus-host disease (GVHD). GVHD is a potentially life-threatening disorder predominantly affecting the skin (Fig 28.2
Stem cell transplantation
Allogeneic and syngeneic (twin) SCT
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oncohema Key
Fastest Oncology & Hematology Insight Engine